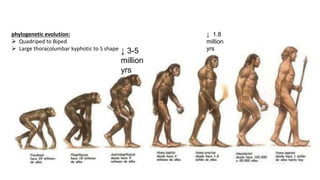
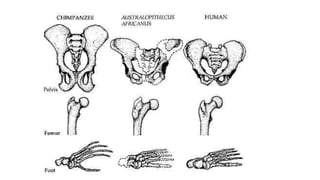
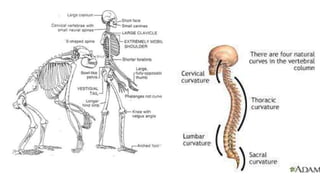
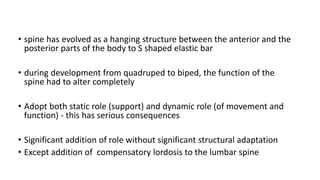
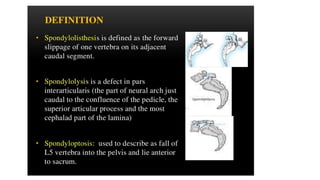
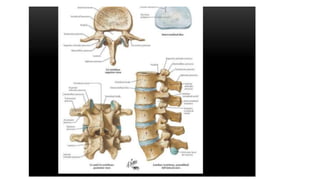
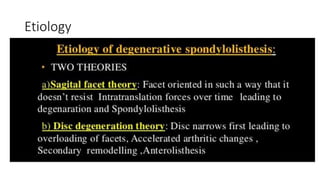
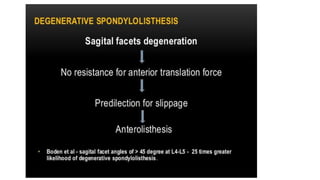
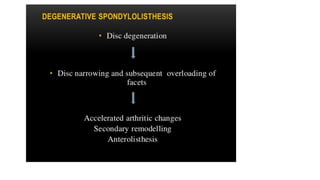
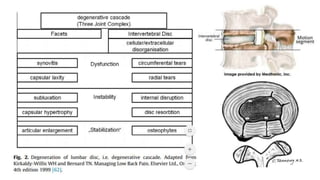
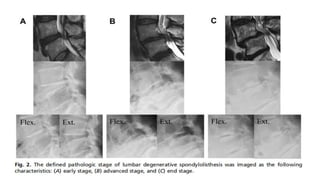
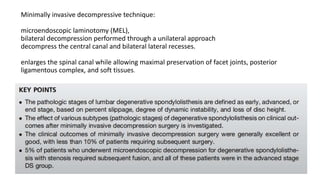
This document discusses lumbar degenerative spondylolisthesis. It begins by covering the phylogenetic evolution of the spine from quadruped to biped posture and how this impacted spinal loading and development. It then reviews recent literature on controversies regarding conservative versus surgical management. Specifically, it summarizes findings from the SPORT, SLIP, and SSSS trials comparing laminectomy alone to laminectomy with fusion. The document concludes by outlining the authors' surgical experience with posterolateral fusion for spondylolisthesis.




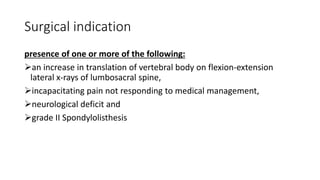
![Patient Baseline Demographic and Clinical Characteristics, N=16
Age (mean ± SD) (y*) 58.8 ±10.5
Sex [n (%)]
Clinical symptomatology
Comorbidity
DOI
FU (Mean±SD) (m**)
F 13 (81.25)
M 3(18.75)
Back pain with caludication 11 (68.75)
Back pain with radiculopathy 5 (31.25)
DM 3 (18.75)
Bed ridden 3 (18.75)
Cushing disease 1(6.25)
(Mean±SD) (m**) 22.06±19.08
13.56±7.15](https://image.slidesharecdn.com/lumbardegenerativespondylolisthesis-200130011002/85/Lumbar-degenerative-spondylolisthesis-60-320.jpg)
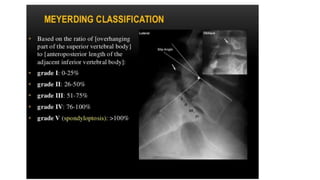
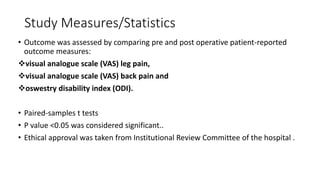
![Mayerding grading
Mortality
Grade I 12 (75)
Grade II 4(25)
L4/5 10 (62.5)
L5/S1 6 (37.5)
1 (6.5)
3(18.75)
0
Note: *y: year,** m: month
Level of spondylolisthesis [n (%)]
Intraoperative complications [n (%)]
Postoperative complications [n (%)]
Dural tear
Wound dehiscence, superfificial infection](https://image.slidesharecdn.com/lumbardegenerativespondylolisthesis-200130011002/85/Lumbar-degenerative-spondylolisthesis-61-320.jpg)