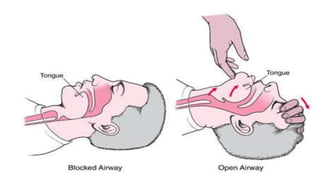
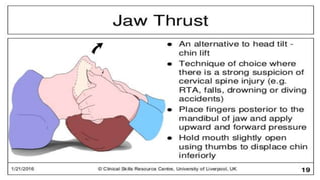
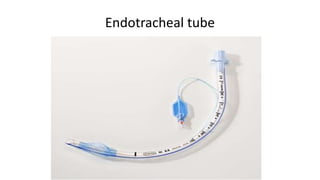
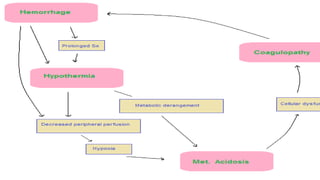
The document discusses polytrauma, Advanced Trauma Life Support (ATLS), and damage control surgery. It defines polytrauma as injuries to at least two body regions with an Abbreviated Injury Scale score of 3 or higher in conjunction with physiological abnormalities. ATLS involves assessing the airway, breathing, circulation, disability, and exposure during the primary survey to address life threats, followed by a secondary survey. Damage control surgery focuses on rapidly controlling hemorrhage, limiting contamination, and temporarily stabilizing fractures to prevent the triad of death from trauma before definitive care.
































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)














