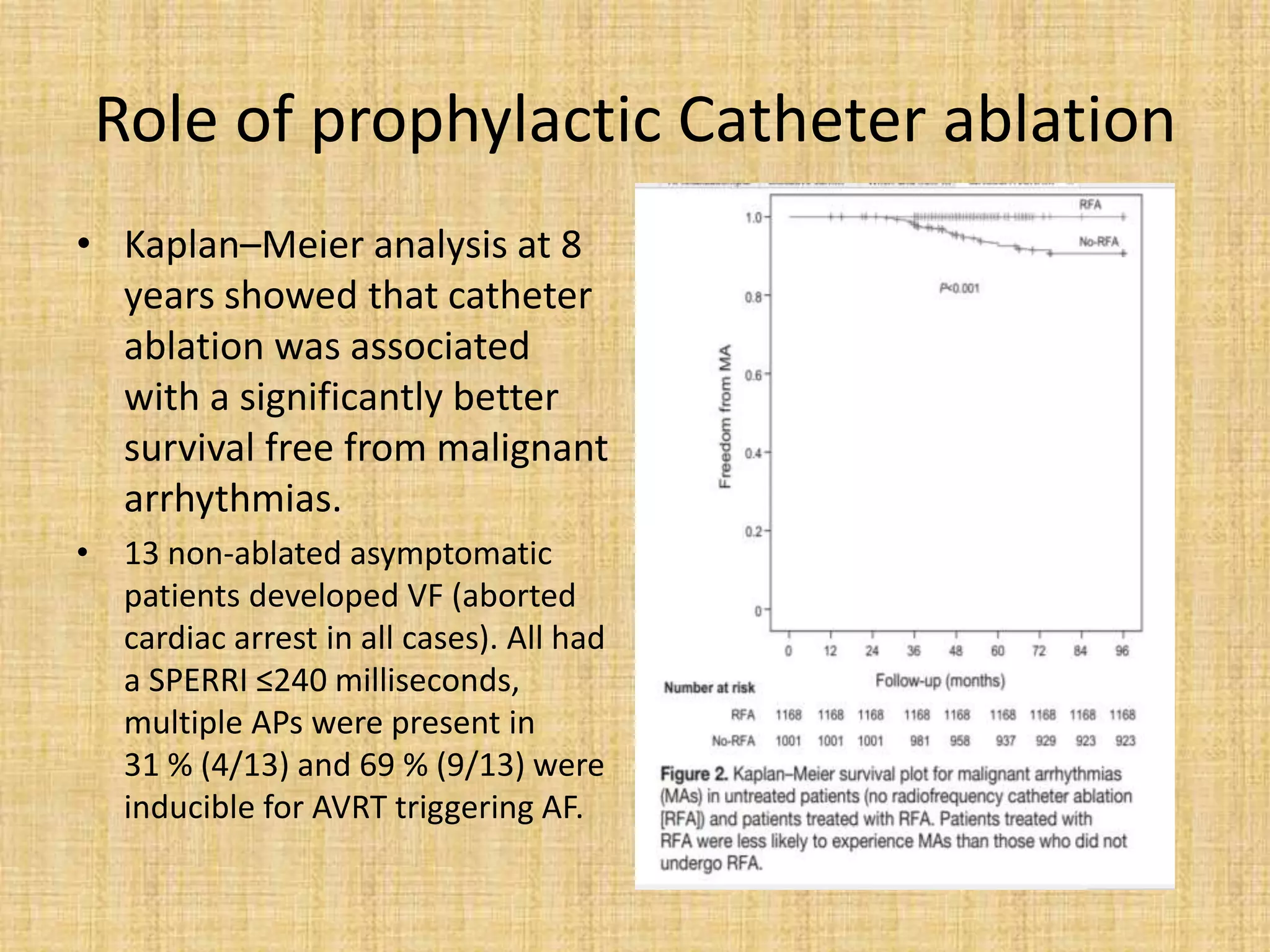
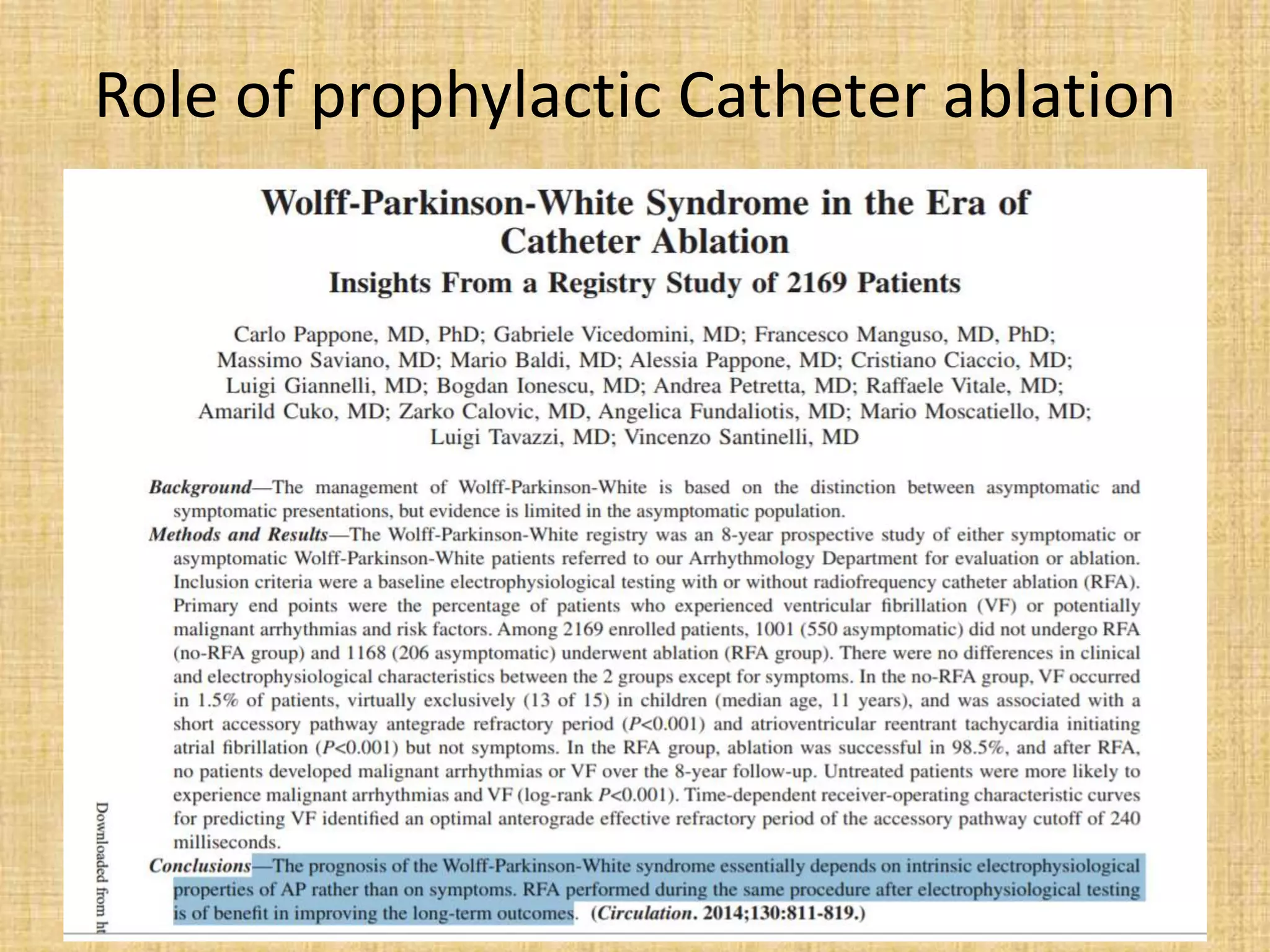
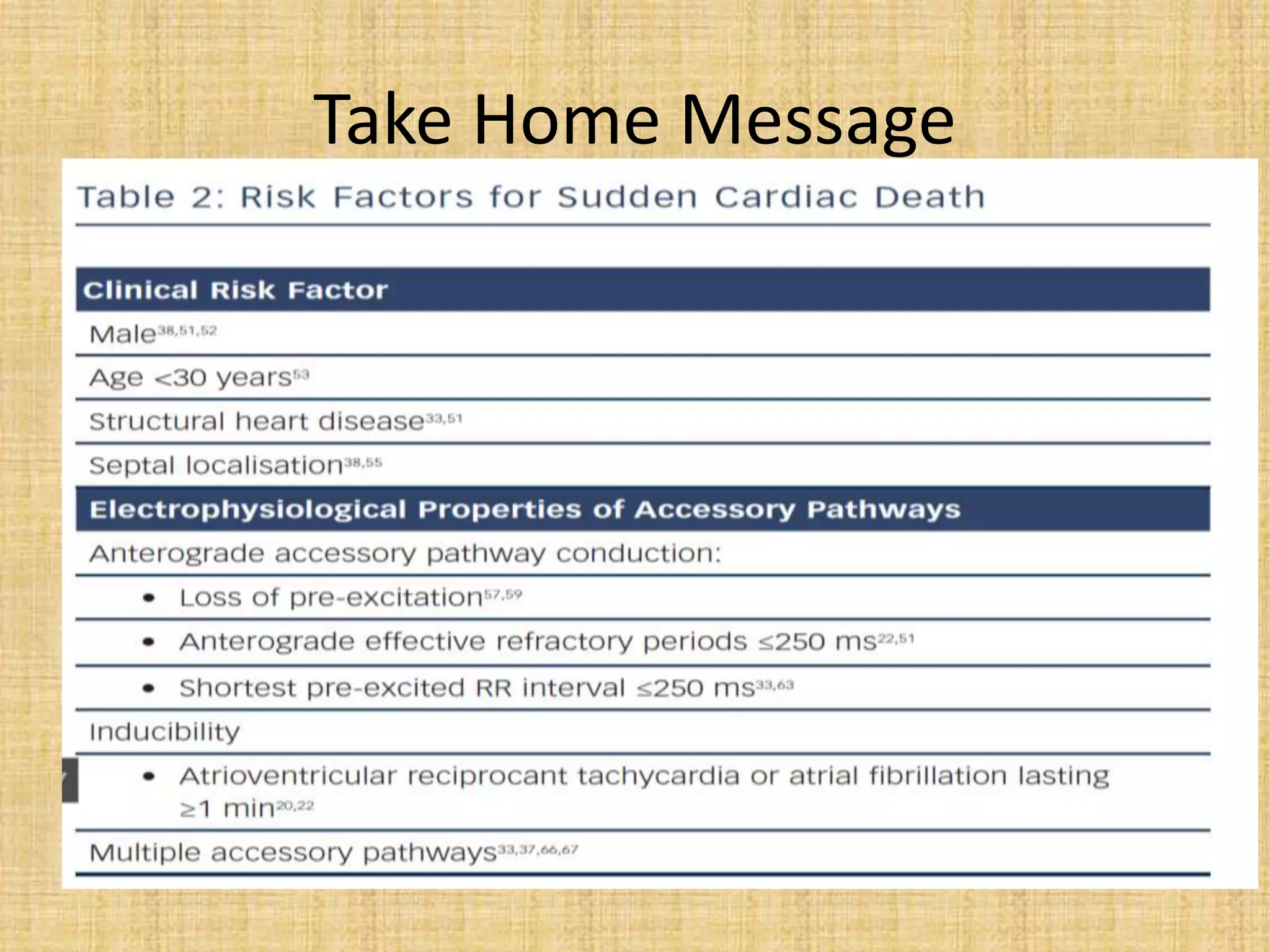
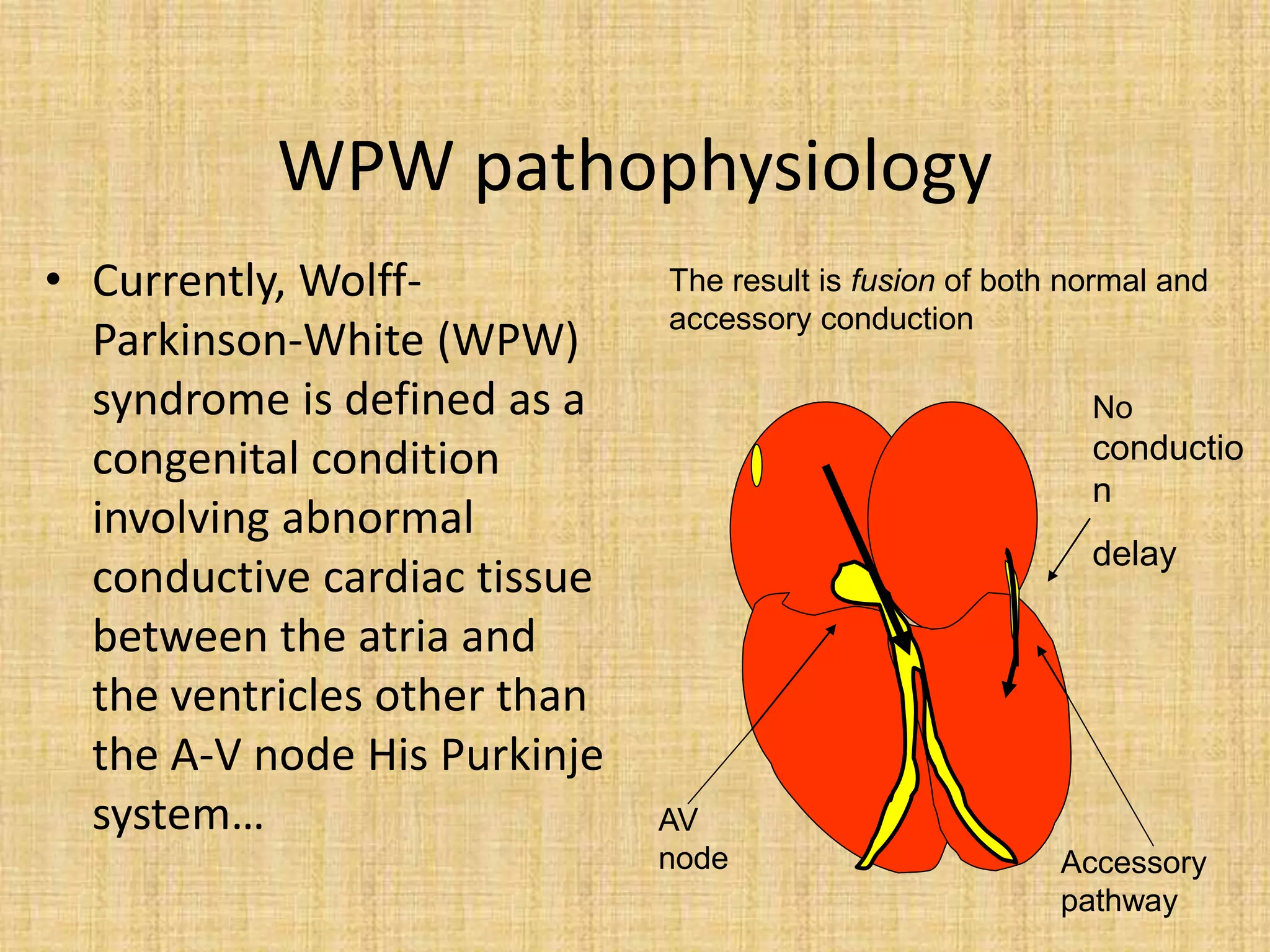
This document discusses the management of asymptomatic Wolff-Parkinson-White (WPW) syndrome. It outlines the risks of sudden cardiac death even in asymptomatic patients and challenges the approach of "leaving the patient alone." The document recommends using risk stratification to identify high-risk asymptomatic patients, such as those with a short accessory pathway effective refractory period (<250ms) or shortest pre-excited RR interval during induced atrial fibrillation (<250ms). For low-risk asymptomatic patients, close monitoring is recommended, while electrophysiological study with potential ablation is recommended for higher risk patients due to the risk of sudden cardiac death. Long-term studies show catheter ablation significantly reduces risks of malignant arrhythmias compared to













![Age in Children
• It was thought that children below 12 years rarely gets AF…
• Pappone et al. in their study [New Ing JM, 2004] of five to 12-year
old WPW children, reported an apparently high incidence of induced
tachycardia (60/165) and spontaneous tachycardia in these children.
One case of sudden death and two cases of ventricular fibrillation
were reported in untreated children, the younger of whom was 10
years old.
• Sarrubi et al 2005, reported in their study a case of sudden death at
the age of 8 yrs.
• It is therefore widely recommended that a pre-excitation syndrome
be assessed from the age of seven years old onwards with no upper
age limit depending on the person’s activities.](https://image.slidesharecdn.com/asymptomaticwpwmanagement-200413224337/75/Asymptomatic-WPW-management-25-2048.jpg)


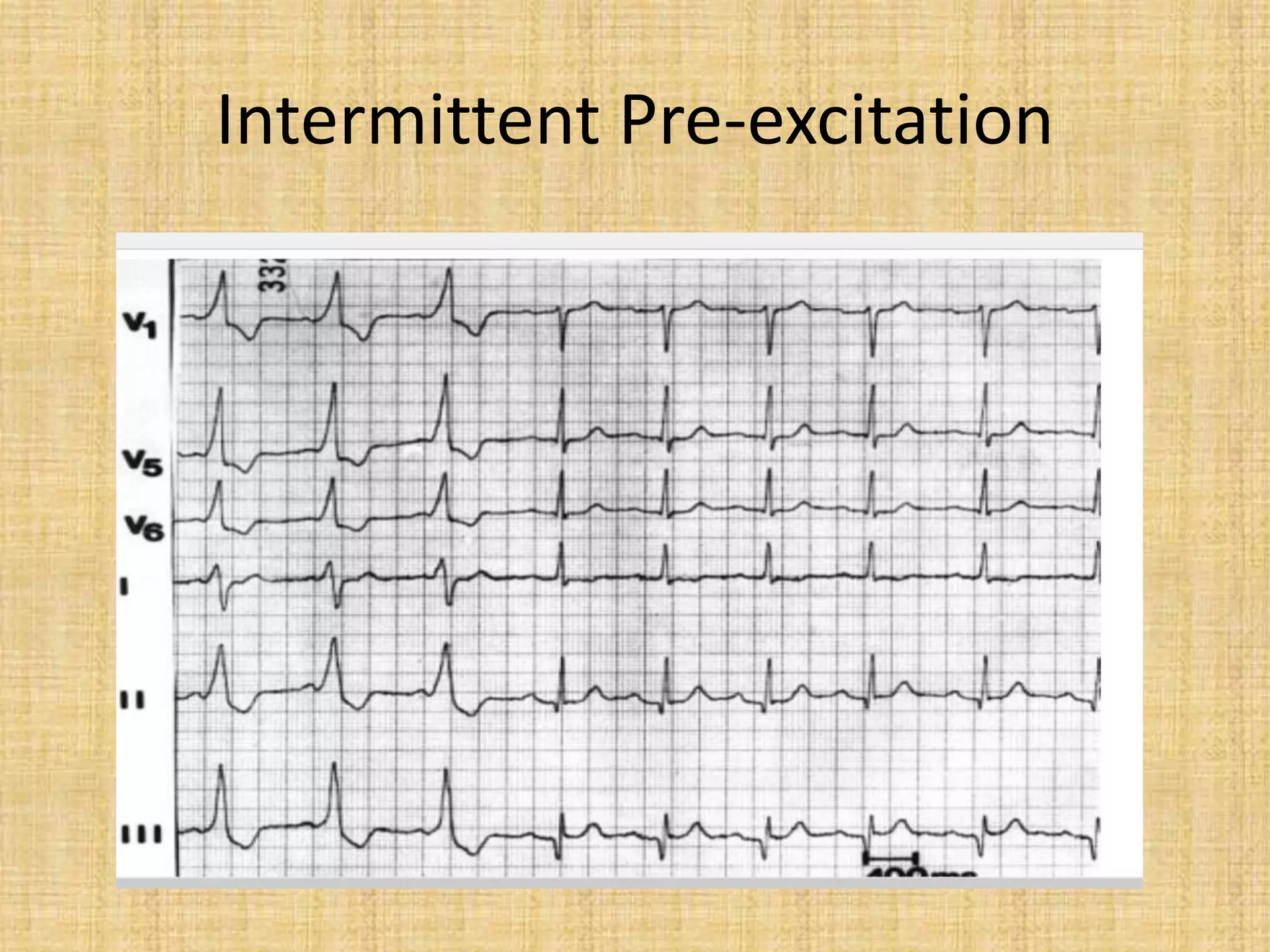
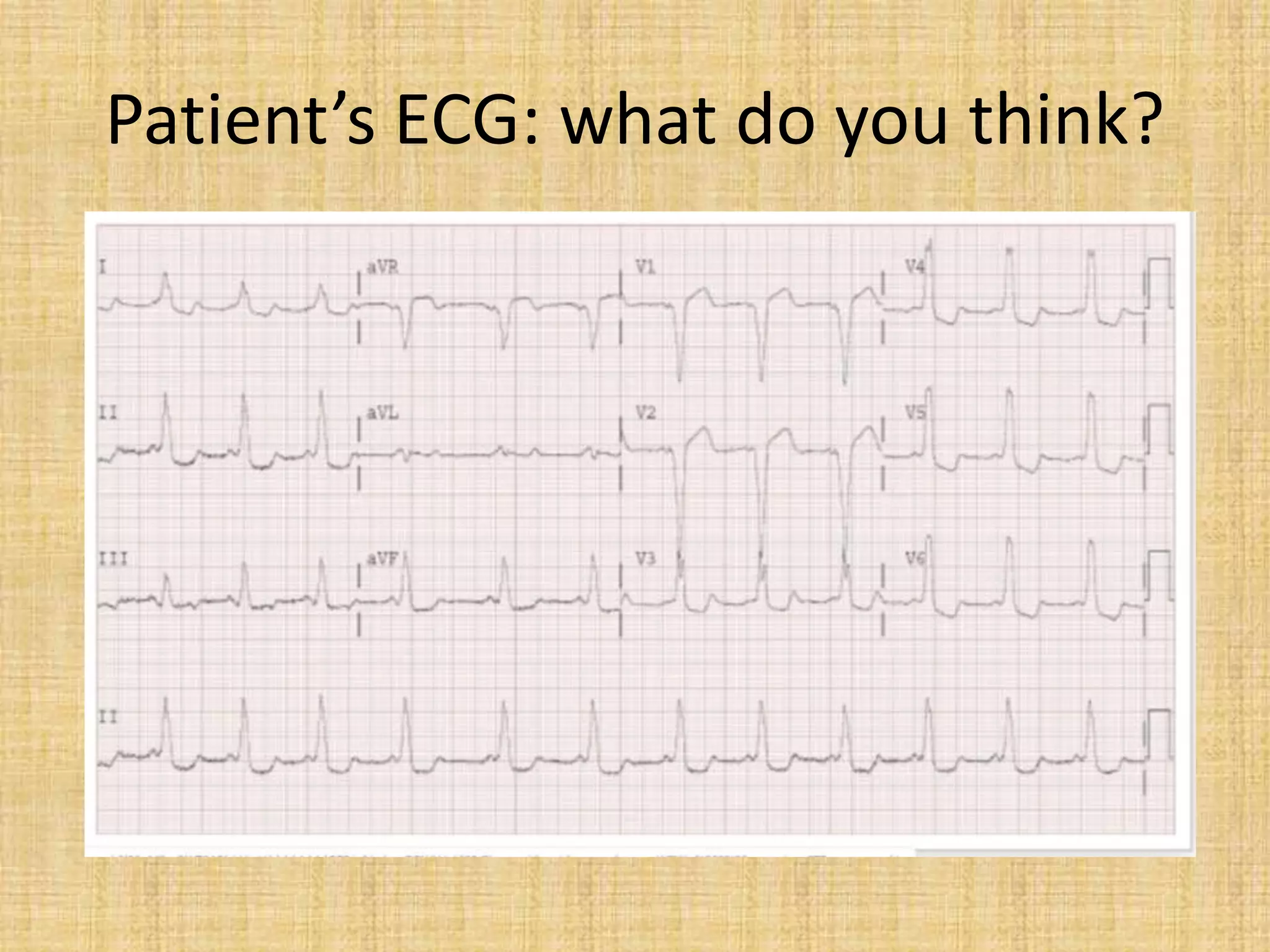
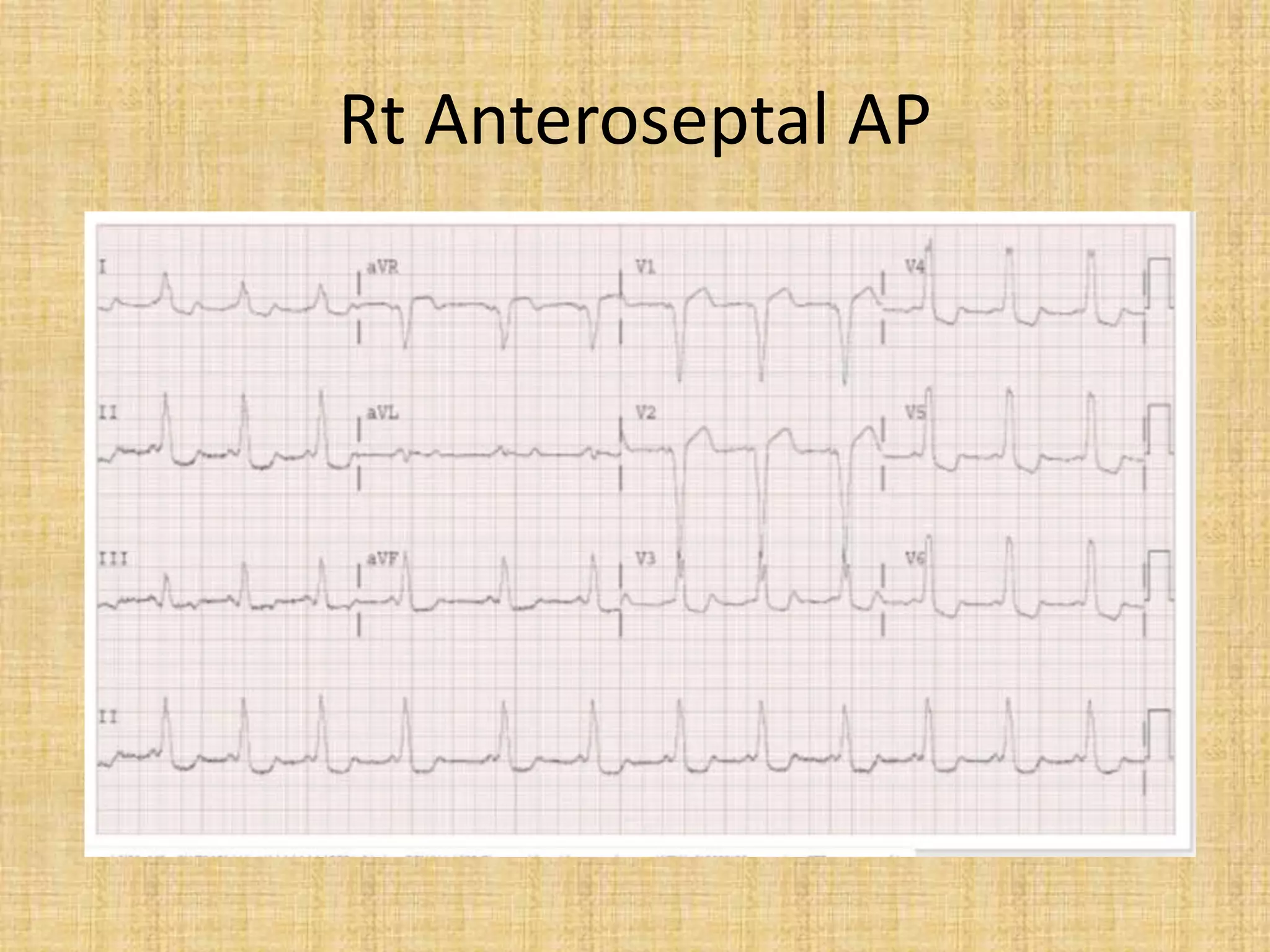
![The resting surface
electrocardiogram (ECG)
• It may suggest a benign form of the
condition if the pre-excitation is
intermittent, although this is not a specific
finding [Kiger et al 2016].
• On the other hand, the presence of more
than one pre-excitation form suggestive of
multiple APs can be a sign of high risk…](https://image.slidesharecdn.com/asymptomaticwpwmanagement-200413224337/75/Asymptomatic-WPW-management-28-2048.jpg)





![Exercise testing
• The exercise test is perhaps the most reliable way of
identifying a benign form of the disorder if the preexcitation
disappears suddenly [Levy et al 1979].
• We must be wary of progressive narrowing of the QRS
complex which may lead to the diagnosis of a false positive
benign WPW and miss a risk of sudden death. This situation
has already been published
• Daubert et al demonstrated that only abrupt and complete
loss of preexcitation during exercise confirmed a long
anterograde APERP. The positive predictive value was 40%
and the negative predictive value was 88%.
(Daubert et al. Am J Cardiol 1986.)](https://image.slidesharecdn.com/asymptomaticwpwmanagement-200413224337/75/Asymptomatic-WPW-management-38-2048.jpg)



![Role of Electrophysiological studies
• Electrophysiological studies were controversial, until 2003 as
until that time identifying malignant forms of the disorder
had not been found to be associated with a true risk of
event in patient follow up.
• It was Pappone et al. [JACC, 2003] who demonstrated in a
large series of 224 adolescents and young adults that 3
patients with rapid induced atrial fibrillation died because
they had declined ablation of their accessory pathway.](https://image.slidesharecdn.com/asymptomaticwpwmanagement-200413224337/75/Asymptomatic-WPW-management-42-2048.jpg)







![Dangerous SPERRI
• Induction of atrial fibrillation conducted
rapidly by the accessory pathway (over
240/min at baseline base state i.e ,250 ms and
over 300/min i.e <200 ms on isoprenaline) can
identify a person with a malignant form of the
disorder.
[Wellens et al, Circulation 2005]](https://image.slidesharecdn.com/asymptomaticwpwmanagement-200413224337/75/Asymptomatic-WPW-management-53-2048.jpg)