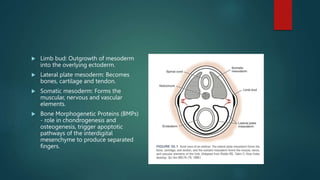
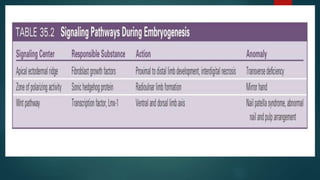
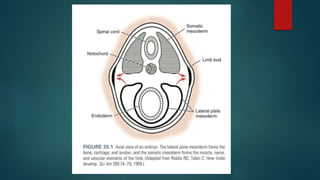
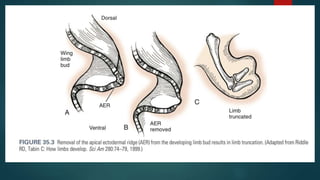
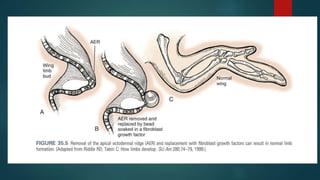
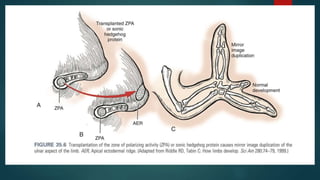
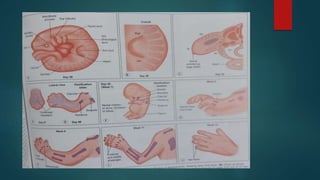
The document discusses the embryology of the upper limb and hand development. It notes that between 5-8 weeks of gestation is the critical period for limb development. The zones of polarizing activity and apical ectodermal ridge play important roles in directing growth. Thumb hypoplasia is often associated with radial deficiencies and other syndromes. The document covers classifications of thumb hypoplasia and radial deficiencies and discusses evaluation and treatment considerations.











![CONGENITAL HAND ANOMALIES PRESENTATION[1].pptxUPDATED 1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/congenitalhandanomaliespresentation1-250730085516-b1c22b4b-thumbnail.jpg?width=640&height=640&fit=bounds)












































