Download as PDF, PPTX
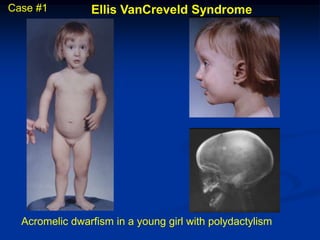

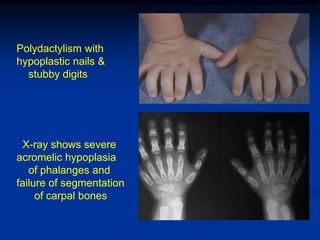

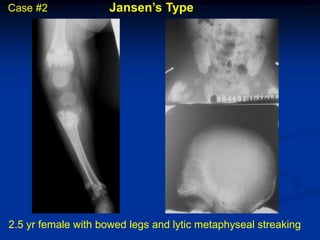
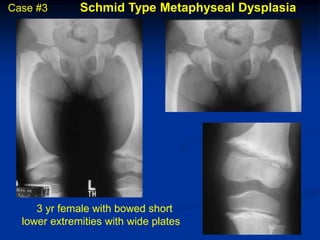
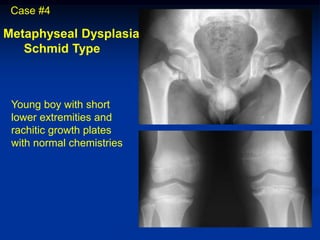
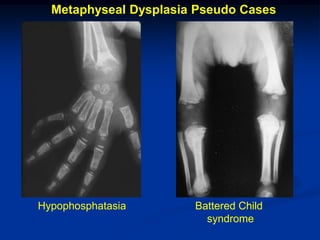


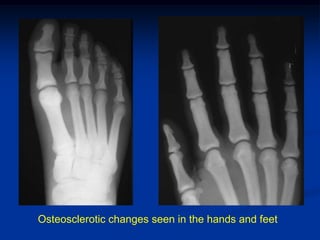

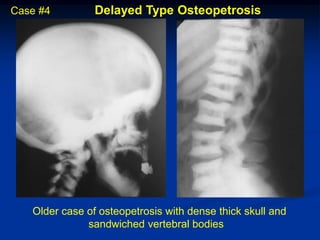
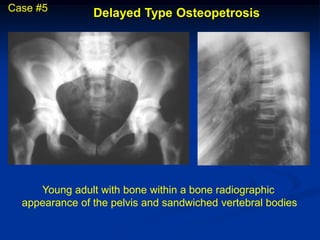
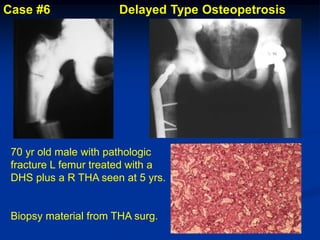


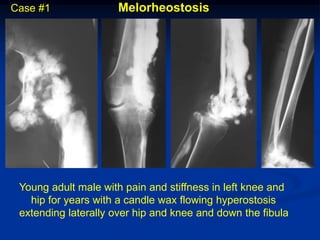
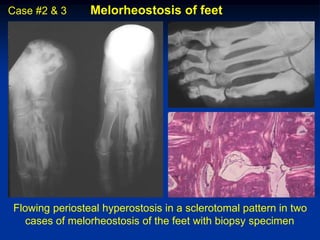
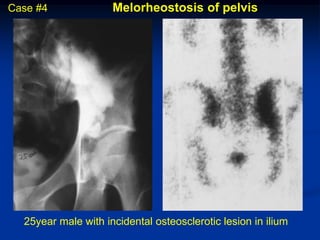
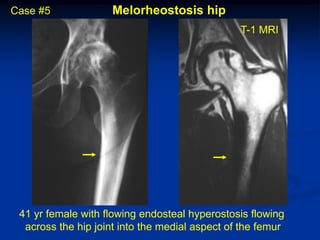












This document summarizes several congenital bone defects. It describes Ellis VanCreveld syndrome, which causes dwarfism, polydactyly, and dental/nail defects. It also discusses several types of metaphyseal dysplasias that result in abnormal growth plate formation and short stature. Osteopetrosis is described as causing excessive bone density due to osteoclast dysfunction. Craniometaphyseal dysplasia causes thinning of long bones. Other conditions mentioned include osteopathia striata, osteopoikilosis, and melorheostosis. Case studies with images are provided to illustrate the radiographic findings of several of these bone diseases.













































































