This document provides a summary of articles across various medical specialties discussed in the April 2015 edition of the UTSW Journal Watch. In the Hepatology section, an article is summarized that finds corticosteroids may be safely used in patients with severe alcoholic hepatitis who present with an upper GI bleed after bleeding is controlled. In Pulmonary/Critical Care, a summary is provided of a trial finding no difference in mortality between early goal-directed therapy and usual care for treating septic shock. The study suggests protocols for goals of care are less important than early antibiotics and fluids. In Nephrology, a meta-analysis summary indicates preoperative use of renin-angiotensin system inhibitors may be linked to
Nivolumab, a programmed death 1 (PD-1) checkpoint inhibitor, was associated with encouraging overall survival in uncontrolled studies involving previously treated patients with advanced renal-cell carcinoma. This randomized, open-label, phase 3 study compared nivolumab with everolimus in patients with renal-cell carcinoma who had received previous treatment.
Nivolumab, a programmed death 1 (PD-1) checkpoint inhibitor, was associated with encouraging overall survival in uncontrolled studies involving previously treated patients with advanced renal-cell carcinoma. This randomized, open-label, phase 3 study compared nivolumab with everolimus in patients with renal-cell carcinoma who had received previous treatment.
Sydney Sexual Health Centre Journal Club presentation by Cherie Desreaux on the British Medical Journal and the Medical Journal of Australia editions published between November 2015 and March 2016.
The Sydney Sexual Health Centre Journal Club allows our team to stay up-to-date with what is being published in the field of sexual health. Staff members take turns to read, review and share the contents of an allocated journal. Journal Club encourages knowledge sharing and discussion about topics raised.
Erectile Dysfunction and Risk Factors in Male Peruvian Hemodialysis Patientsasclepiuspdfs
Introduction: Erectile dysfunction (ED) is a common condition in patients with renal disease, but little is known about the prevalence of ED in some specific groups of patients such as Peruvian hemodialysis (HD) patients. Materials and Methods: A cross‑sectional study was conducted to determine the frequency of ED in HD patients (n = 390) in Lima, Peru. The prevalence and severity of ED were assessed using the International Index of Erectile Function with the validated Peruvian version. The dependence of ED on independent variables was evaluated by logistic regression. P ≤ 0.05 was regarded as statistically significant.
The study to measure the level of serum annexin V in patients with renal hype...inventionjournals
ABSTRACT : Renovascular hypertension reflects the causal relation between anatomically evident arterial occlusive disease and elevated blood pressure. The coexistence of renal arterial vascular disease and hypertension roughly defines this type of nonessential hypertension. The aim of this study was to measure the level of serum Anti-Annexin V antibodies in patients with renal hypertension. Methods. This study was conducted on 115 patients, diagnosed with renal hypertension and hypertension. Informed consents were obtained from the patients and the study was approved by the Kharkiv National Medical University ethics committee. Ten healthy age and sex matched volunteers were included as a control group. All patients and controls were subjected to the following full history taking and thorough clinical examination. Routine laboratory testing included a complete blood count, and erythrocyte sedimentation rate (ESR) and kidney function tests (blood urea nitrogen and serum creatinine). Immunological tests for antinuclear antibody (ANA) and anticentromere antibodies (ACA) was performed by the indirect immunofluorescence technique. AntiScl-70 (anti-topoisomerase antibodies) and anticardiolipin antibodies (ACA: IgG and IgM) were tested using the ELISA technique. The anti-annexin V antibodies titre used the ZYMUTEST anti-Annexin IgG ELISA kit. [Hyphen-BioMed, France.]: to measure the IgG isotype of auto-antibodies to annexin V in human serum. Results. Anti-annexin V antibodies were present in 75% of patients (mean 83.46 ± 22.44 AU/mL) vs. 0% in the controls (mean 3.94 ± 4.5 AU/mL). Comparison between patients and controls as regards levels of anti-annexin V showed a highly significant difference (P < 0.001). Furthermore, correlation of anti-annexin V titres with the disease activity score in the patient group showed a statistically significant positive correlation (r = 0.51, P < 0.05).In addition, the anti-annexin V antibody titres in this study showed a highly significant positive correlation with ACL antibodies (r = 0.74, P < 0.001). Patients with antiphospholipid syndrome (APS) have been known to have a higher frequency of anti-annexin V antibodies, and thrombotic events have been reported more frequently in patients with positive anti-annexin V antibodies. Furthermore, inhibition of annexin V binding to negatively charged phospholipids may be an additional pathogenic mechanism of APS.
Аллопуринол и прогрессирование ХБП и кардиоваскулярные события. РКИ / Allopur...hivlifeinfo
Allopurinol and Progression of CKD and Cardiovascular Events- Long-term Follow-up of a Randomized Clinical Trial.Am J Kidney Dis. 2015 Apr
Background:Asymptomatic hyperuricemia increases renal and cardiovascular (CV) risk. We previously
conducted a 2-year, single-blind, randomized, controlled trial of allopurinol treatment that showed improved
estimated glomerular filtration rate and reduced CV risk.
Study Design:Post hoc analysis of a long-term follow-up after completion of the 2-year trial.
Setting & Participants:113 participants (57 in the allopurinol group and 56 in the control group) initially
followed up for 2 years and 107 participants followed up to 5 additional years.
Intervention: Continuation of allopurinol treatment, 100 mg/d, or standard treatment.
Outcome:Renal event (defined as starting dialysis therapy and/or doubling serum creatinine and/or$50%
decrease in estimated estimated glomerular filtration rate) and CV events (defined as myocardial infarction,
coronary revascularization or angina pectoris, congestive heart failure, cerebrovascular disease, and peripheral vascular disease).
Results:During initial follow-up, there were 2 renal and 7 CV events in the allopurinol group compared with
6 renal and 15 CV events in the control group. In the long-term follow-up period, 12 of 56 participants taking
allopurinol stopped treatment and 10 of 51 control participants received allopurinol. During long-term follow-up,
an additional 7 and 9 participants in the allopurinol group experienced a renal or CV event, respectively, and an
additional 18 and 8 participants in the control group experienced a renal or CV event, respectively. Thus,
during the initial and long-term follow-up (median, 84 months), 9 patients in the allopurinol group had a
renal event compared with 24 patients in the control group (HR, 0.32; 95% CI, 0.15-0.69; P50.004;
adjusted for age, sex, baseline kidney function, uric acid level, and renin-angiotensin-aldosterone system
blockers). Overall, 16 patients treated with allopurinol experienced CV events compared with 23 in the
control group (HR, 0.43; 95% CI, 0.21-0.88;P50.02; adjusted for age, sex, and baseline kidney function).
Limitations:Small sample size, single center, not double blind, post hoc follow-up and analysis.
Conclusions: Long-term treatment with allopurinol may slow the rate of progression of kidney disease and
reduce CV risk.
Sydney Sexual Health Centre Journal Club presentation by Cherie Desreaux on the British Medical Journal and the Medical Journal of Australia editions published between November 2015 and March 2016.
The Sydney Sexual Health Centre Journal Club allows our team to stay up-to-date with what is being published in the field of sexual health. Staff members take turns to read, review and share the contents of an allocated journal. Journal Club encourages knowledge sharing and discussion about topics raised.
Erectile Dysfunction and Risk Factors in Male Peruvian Hemodialysis Patientsasclepiuspdfs
Introduction: Erectile dysfunction (ED) is a common condition in patients with renal disease, but little is known about the prevalence of ED in some specific groups of patients such as Peruvian hemodialysis (HD) patients. Materials and Methods: A cross‑sectional study was conducted to determine the frequency of ED in HD patients (n = 390) in Lima, Peru. The prevalence and severity of ED were assessed using the International Index of Erectile Function with the validated Peruvian version. The dependence of ED on independent variables was evaluated by logistic regression. P ≤ 0.05 was regarded as statistically significant.
The study to measure the level of serum annexin V in patients with renal hype...inventionjournals
ABSTRACT : Renovascular hypertension reflects the causal relation between anatomically evident arterial occlusive disease and elevated blood pressure. The coexistence of renal arterial vascular disease and hypertension roughly defines this type of nonessential hypertension. The aim of this study was to measure the level of serum Anti-Annexin V antibodies in patients with renal hypertension. Methods. This study was conducted on 115 patients, diagnosed with renal hypertension and hypertension. Informed consents were obtained from the patients and the study was approved by the Kharkiv National Medical University ethics committee. Ten healthy age and sex matched volunteers were included as a control group. All patients and controls were subjected to the following full history taking and thorough clinical examination. Routine laboratory testing included a complete blood count, and erythrocyte sedimentation rate (ESR) and kidney function tests (blood urea nitrogen and serum creatinine). Immunological tests for antinuclear antibody (ANA) and anticentromere antibodies (ACA) was performed by the indirect immunofluorescence technique. AntiScl-70 (anti-topoisomerase antibodies) and anticardiolipin antibodies (ACA: IgG and IgM) were tested using the ELISA technique. The anti-annexin V antibodies titre used the ZYMUTEST anti-Annexin IgG ELISA kit. [Hyphen-BioMed, France.]: to measure the IgG isotype of auto-antibodies to annexin V in human serum. Results. Anti-annexin V antibodies were present in 75% of patients (mean 83.46 ± 22.44 AU/mL) vs. 0% in the controls (mean 3.94 ± 4.5 AU/mL). Comparison between patients and controls as regards levels of anti-annexin V showed a highly significant difference (P < 0.001). Furthermore, correlation of anti-annexin V titres with the disease activity score in the patient group showed a statistically significant positive correlation (r = 0.51, P < 0.05).In addition, the anti-annexin V antibody titres in this study showed a highly significant positive correlation with ACL antibodies (r = 0.74, P < 0.001). Patients with antiphospholipid syndrome (APS) have been known to have a higher frequency of anti-annexin V antibodies, and thrombotic events have been reported more frequently in patients with positive anti-annexin V antibodies. Furthermore, inhibition of annexin V binding to negatively charged phospholipids may be an additional pathogenic mechanism of APS.
Аллопуринол и прогрессирование ХБП и кардиоваскулярные события. РКИ / Allopur...hivlifeinfo
Allopurinol and Progression of CKD and Cardiovascular Events- Long-term Follow-up of a Randomized Clinical Trial.Am J Kidney Dis. 2015 Apr
Background:Asymptomatic hyperuricemia increases renal and cardiovascular (CV) risk. We previously
conducted a 2-year, single-blind, randomized, controlled trial of allopurinol treatment that showed improved
estimated glomerular filtration rate and reduced CV risk.
Study Design:Post hoc analysis of a long-term follow-up after completion of the 2-year trial.
Setting & Participants:113 participants (57 in the allopurinol group and 56 in the control group) initially
followed up for 2 years and 107 participants followed up to 5 additional years.
Intervention: Continuation of allopurinol treatment, 100 mg/d, or standard treatment.
Outcome:Renal event (defined as starting dialysis therapy and/or doubling serum creatinine and/or$50%
decrease in estimated estimated glomerular filtration rate) and CV events (defined as myocardial infarction,
coronary revascularization or angina pectoris, congestive heart failure, cerebrovascular disease, and peripheral vascular disease).
Results:During initial follow-up, there were 2 renal and 7 CV events in the allopurinol group compared with
6 renal and 15 CV events in the control group. In the long-term follow-up period, 12 of 56 participants taking
allopurinol stopped treatment and 10 of 51 control participants received allopurinol. During long-term follow-up,
an additional 7 and 9 participants in the allopurinol group experienced a renal or CV event, respectively, and an
additional 18 and 8 participants in the control group experienced a renal or CV event, respectively. Thus,
during the initial and long-term follow-up (median, 84 months), 9 patients in the allopurinol group had a
renal event compared with 24 patients in the control group (HR, 0.32; 95% CI, 0.15-0.69; P50.004;
adjusted for age, sex, baseline kidney function, uric acid level, and renin-angiotensin-aldosterone system
blockers). Overall, 16 patients treated with allopurinol experienced CV events compared with 23 in the
control group (HR, 0.43; 95% CI, 0.21-0.88;P50.02; adjusted for age, sex, and baseline kidney function).
Limitations:Small sample size, single center, not double blind, post hoc follow-up and analysis.
Conclusions: Long-term treatment with allopurinol may slow the rate of progression of kidney disease and
reduce CV risk.
Association and prevalence of different comorbidities in hypertension and management with focus guidelines with benefits & choice of different antihypertensives in different comorbidities.
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
MANAGEMENT OF ATRIOVENTRICULAR CONDUCTION BLOCK.pdfJim Jacob Roy
Cardiac conduction defects can occur due to various causes.
Atrioventricular conduction blocks ( AV blocks ) are classified into 3 types.
This document describes the acute management of AV block.
Flu Vaccine Alert in Bangalore Karnatakaaddon Scans
As flu season approaches, health officials in Bangalore, Karnataka, are urging residents to get their flu vaccinations. The seasonal flu, while common, can lead to severe health complications, particularly for vulnerable populations such as young children, the elderly, and those with underlying health conditions.
Dr. Vidisha Kumari, a leading epidemiologist in Bangalore, emphasizes the importance of getting vaccinated. "The flu vaccine is our best defense against the influenza virus. It not only protects individuals but also helps prevent the spread of the virus in our communities," he says.
This year, the flu season is expected to coincide with a potential increase in other respiratory illnesses. The Karnataka Health Department has launched an awareness campaign highlighting the significance of flu vaccinations. They have set up multiple vaccination centers across Bangalore, making it convenient for residents to receive their shots.
To encourage widespread vaccination, the government is also collaborating with local schools, workplaces, and community centers to facilitate vaccination drives. Special attention is being given to ensuring that the vaccine is accessible to all, including marginalized communities who may have limited access to healthcare.
Residents are reminded that the flu vaccine is safe and effective. Common side effects are mild and may include soreness at the injection site, mild fever, or muscle aches. These side effects are generally short-lived and far less severe than the flu itself.
Healthcare providers are also stressing the importance of continuing COVID-19 precautions. Wearing masks, practicing good hand hygiene, and maintaining social distancing are still crucial, especially in crowded places.
Protect yourself and your loved ones by getting vaccinated. Together, we can help keep Bangalore healthy and safe this flu season. For more information on vaccination centers and schedules, residents can visit the Karnataka Health Department’s official website or follow their social media pages.
Stay informed, stay safe, and get your flu shot today!
- Video recording of this lecture in English language: https://youtu.be/lK81BzxMqdo
- Video recording of this lecture in Arabic language: https://youtu.be/Ve4P0COk9OI
- Link to download the book free: https://nephrotube.blogspot.com/p/nephrotube-nephrology-books.html
- Link to NephroTube website: www.NephroTube.com
- Link to NephroTube social media accounts: https://nephrotube.blogspot.com/p/join-nephrotube-on-social-media.html
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
New Directions in Targeted Therapeutic Approaches for Older Adults With Mantl...i3 Health
i3 Health is pleased to make the speaker slides from this activity available for use as a non-accredited self-study or teaching resource.
This slide deck presented by Dr. Kami Maddocks, Professor-Clinical in the Division of Hematology and
Associate Division Director for Ambulatory Operations
The Ohio State University Comprehensive Cancer Center, will provide insight into new directions in targeted therapeutic approaches for older adults with mantle cell lymphoma.
STATEMENT OF NEED
Mantle cell lymphoma (MCL) is a rare, aggressive B-cell non-Hodgkin lymphoma (NHL) accounting for 5% to 7% of all lymphomas. Its prognosis ranges from indolent disease that does not require treatment for years to very aggressive disease, which is associated with poor survival (Silkenstedt et al, 2021). Typically, MCL is diagnosed at advanced stage and in older patients who cannot tolerate intensive therapy (NCCN, 2022). Although recent advances have slightly increased remission rates, recurrence and relapse remain very common, leading to a median overall survival between 3 and 6 years (LLS, 2021). Though there are several effective options, progress is still needed towards establishing an accepted frontline approach for MCL (Castellino et al, 2022). Treatment selection and management of MCL are complicated by the heterogeneity of prognosis, advanced age and comorbidities of patients, and lack of an established standard approach for treatment, making it vital that clinicians be familiar with the latest research and advances in this area. In this activity chaired by Michael Wang, MD, Professor in the Department of Lymphoma & Myeloma at MD Anderson Cancer Center, expert faculty will discuss prognostic factors informing treatment, the promising results of recent trials in new therapeutic approaches, and the implications of treatment resistance in therapeutic selection for MCL.
Target Audience
Hematology/oncology fellows, attending faculty, and other health care professionals involved in the treatment of patients with mantle cell lymphoma (MCL).
Learning Objectives
1.) Identify clinical and biological prognostic factors that can guide treatment decision making for older adults with MCL
2.) Evaluate emerging data on targeted therapeutic approaches for treatment-naive and relapsed/refractory MCL and their applicability to older adults
3.) Assess mechanisms of resistance to targeted therapies for MCL and their implications for treatment selection
Couples presenting to the infertility clinic- Do they really have infertility...Sujoy Dasgupta
Dr Sujoy Dasgupta presented the study on "Couples presenting to the infertility clinic- Do they really have infertility? – The unexplored stories of non-consummation" in the 13th Congress of the Asia Pacific Initiative on Reproduction (ASPIRE 2024) at Manila on 24 May, 2024.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
Ethanol (CH3CH2OH), or beverage alcohol, is a two-carbon alcohol
that is rapidly distributed in the body and brain. Ethanol alters many
neurochemical systems and has rewarding and addictive properties. It
is the oldest recreational drug and likely contributes to more morbidity,
mortality, and public health costs than all illicit drugs combined. The
5th edition of the Diagnostic and Statistical Manual of Mental Disorders
(DSM-5) integrates alcohol abuse and alcohol dependence into a single
disorder called alcohol use disorder (AUD), with mild, moderate,
and severe subclassifications (American Psychiatric Association, 2013).
In the DSM-5, all types of substance abuse and dependence have been
combined into a single substance use disorder (SUD) on a continuum
from mild to severe. A diagnosis of AUD requires that at least two of
the 11 DSM-5 behaviors be present within a 12-month period (mild
AUD: 2–3 criteria; moderate AUD: 4–5 criteria; severe AUD: 6–11 criteria).
The four main behavioral effects of AUD are impaired control over
drinking, negative social consequences, risky use, and altered physiological
effects (tolerance, withdrawal). This chapter presents an overview
of the prevalence and harmful consequences of AUD in the U.S.,
the systemic nature of the disease, neurocircuitry and stages of AUD,
comorbidities, fetal alcohol spectrum disorders, genetic risk factors, and
pharmacotherapies for AUD.
2. Page | 2
Hepatology
Corticosteroids in severe alcoholic hepatitis after recent upper GI
bleed
Dr. Jan Petrasek reviewing Rudler et al., J Hepatol. 2015 Apr;62(4):816-21.
10.1016/j.jhep.2014.11.003. Epub 2014 Nov 11.
Summary: GI bleed, if effectively controlled, should not be a contraindication to
steroids in severe alcoholic hepatitis
Commentary: Both AASLD (American Association for the Study of Liver Disease)
and EASL (European Association for the Study of the Liver) guidelines specify that
patients with severe alcoholic hepatitis with recent upper GI bleed should not
receive corticosteroid treatment. The reason for this may be a carryover from
clinical trials performed in the 1970’s and 1980’s in which patients with upper GI
bleeding were excluded due to the belief that corticosteroids caused gastroduodenal
ulcers and also because no effective treatment of upper GI bleeding existed at that
time. Since then, however, much has changed, including advent of proton pump
inhibitors, endoscopic treatment of variceal bleeding and transjugular
portosystemic shunting.
In this issue of Journal of Hepatology, Rudler et al.have published the results of a
retrospective analysis of survival among patients with severe alcoholic hepatitis
(Maddrey’s Discriminant Function ≥ 32) who presented to hospital with upper GI
bleed and compared them with patients with severe alcoholic hepatitis without GI
bleeding. A total of 48 patients with upper GI bleed and 47 patients without GI bleed
were analyzed. The two groups did not differ in presence of alcoholic hepatitis on
biopsy (approximately 80%) or Maddrey’s Discriminant Function (63 and 65,
respectively). After stabilization and effective endoscopic bleeding control, both
groups were started on corticosteroids (40 mg of prednisolone daily for 28 days).
The 6-month survival was similar in both groups (74% vs. 70%). The probability of
developing an infection after starting corticosteroids was lower among subjects with
upper GI bleed (24%) as compared with subjects without upper GI bleed (45%).
This was attributable to the effect of antibiotic therapy (ceftriaxone) which is
mandated in patients with acute GI bleed. If validated in prospective trials, this data
indicate that patients with severe alcoholic hepatitis presenting with GI bleed may
be safely treated with corticosteroids after achieving effective bleeding control.
Link Out Via UTSW
3. Page | 3
Serum ammonia level for the evaluation of hepatic
encephalopathy
Dr. Jan Petrasek reviewing Ge et al., JAMA. 2014 Aug 13;312(6):643-4.
Summary: Limited value of ammonia levels in liver diseases other than fulminant
liver failure
Commentary: In this JAMA Diagnostic Test Interpretation article, Ge et al. review
the utility of serum ammonia levels in patients with hepatic encephalopathy. It is
common for ammonia levels to be obtained during the evaluation of chronic liver
disease. However, the evidence does not support ammonia measurement under
these circumstances. Hepatic encephalopathy is a clinical, not laboratory diagnosis,
and normal ammonia level does not exclude a diagnosis of hepatic encephalopathy,
nor does an elevated ammonia level establish a diagnosis of hepatic encephalopathy.
Blood ammonia levels correlate poorly with the grade of hepatic encephalopathy in
patients with chronic liver disease. The only clinical utility for measurement of
serum ammonia levels is in patients with fulminant liver failure because ammonia
levels correlate with the severity of encephalopathy and elevated levels greater than
150 to 200 μmol/liter are predictive of cerebral edema.
Link out Via UTSW
4. Page | 4
Rheumatology
Extended report: Prediction of cardiovascular risk in rheumatoid
arthritis: performance of original and adapted SCORE algorithms
Dr. Brian Skaug reviewing Arts, et al. Ann Rheum Dis. 2015 Feb 17. pii: annrheumdis-
2014-206879. doi: 10.1136/annrheumdis-2014-206879
Summary: Efforts toward an accurate cardiovascular risk assessment in
rheumatoid arthritis patients
Commentary: Rheumatoid arthritis (RA) confers an elevated risk of cardiovascular
disease (CVD) and CVD-related mortality that cannot be fully explained by
traditional risk factors such as age, lipid values, smoking, and hypertension. To
account for this risk the European League Against Rheumatism (EULAR) has
recommended a 1.5x multiplication factor to CVD risk scores for RA patients with
two of three criteria (disease duration >10 years, + RF and/or anti-CCP antibodies,
or extra-articular manifestations). However the benefit of incorporating this
recommendation is not supported by strong evidence. Therefore development of an
RA-specific CVD risk prediction algorithm is desirable.
In this report the authors tested whether variables such as RF and anti-CCP
antibodies, inflammatory biomarkers, and clinical disease activity assessments
could improve the predictive ability of the systematic coronary risk evaluation
(SCORE), which is a widely used algorithm in Europe similar to the Framingham
score used more commonly in the US. They compared the ability of an adapted
algorithm to the traditional SCORE algorithm for their ability to predict fatal and
non-fatal cardiac events in a large European cohort of RA patients with no CVD at
baseline. Unfortunately the authors’ adapted algorithm did not show an increased
ability to identify patients at risk for cardiac events compared to the traditional
SCORE algorithm. Similar to the traditional SCORE algorithm, the adapted algorithm
tended to underestimate the risk of cardiac events in those with low scores, and
overestimate the risk in those with high scores. Their results highlight a gap in our
ability to predict cardiac events in RA patients even when RA-related variables are
taken into account. This difficulty may be due to an inadequate understanding of
CVD pathogenesis in patients with autoimmune/inflammatory disease. Future
research on CVD pathogenesis in RA patients could reveal which variables might
better predict CVD risk.
Link Out Via UTSW
5. Page | 5
Pulmonary/Critical Care
Trial of Early, Goal-Directed Resuscitation for Septic Shock [The
Protocolised Management in Sepsis (ProMISe) Trial]
Dr. James Galloway reviewing Mouncey PR et al. N Engl J Med. 2015;372(14):1301-11.
Summary: If patients are identified early in sepsis or septic shock and given
appropriate antibiotics fluids early, then the protocol used afterwards, Early goal
directed therapy, protocol, or usual care is less important. Patients do not need CVP
or SV02 monitoring to improve outcomes.
Commentary: This is the third of three recent trials (with ARISE and ProCESS)
comparing the effect of the "early, goal-directed therapy (EGDT)" protocol with
current usual care on mortality in sepsis. The other two trials demonstrated no
mortality benefit with EGDT at 60 days, but neither trial could rule-out a possible
8% ARR in 90-day mortality for EGDT. ProMISe was designed with 80% power to
detect this outcome. It also included a cost-effectiveness analysis.
ProMISe is a randomized, controlled trial conducted at 56 hospitals across England.
Patients were randomized within 6 hours of presentation to the ED and within 2
hours of meeting the inclusion criteria: >= 18 years of age with 2 or more SIRS
criteria, known or presumed infection, and either hypotension (SBP<90 or MAP<65)
refractory to 1L of IV fluids or blood lactate >= 4 mmol/L.
1260 patients underwent randomization; fewer than 1% was lost to follow up.
Patients were similar at baseline with respect to presence of refractory hypotension,
lactate level, illness severity (as measured by Apache II and similar scores),
comorbidities, and source of infection. In general, patients were treated similarly
between the two groups. All patients received empiric antibiotic therapy prior to
randomization. A similar number of patients in each group (97%) received IV fluids
prior to randomization (median of 2L in each group); it is important to note that the
groups received similar volumes of fluid in the 1st 6 hours, which was different from
the original River's study, where early fluid resuscitation was less aggressive. After
the 1st 6 hours of EGDT vs usual care, care was at the discretion of the treating
clinician.
Intention-to-treat analysis showed no difference in 90-day mortality between EGDT
and usual care (RR 1.01 [95% C.I. 0.85-1.20; P=0.90]; ARR -0.3% [95% C.I. -5.7%-
4.7%]). Patients in the EGDT group had worse organ failure scores, longer ICU stays,
and were subjected to greater treatment intensity (more total IV fluids, vasoactive
drugs, and red blood cell transfusions). Adherence to the EGDT protocol was good
(86-95%) and analysis disclosed no "learning curve effect" to explain the lack of a
positive result. There was no significant difference in adverse events or health-
related quality-of-life. The probability that EGDT was cost-effective was <20%.
6. Page | 6
This study has several limitations. First, blinding was not possible, although this was
also the case in ProCESS, ARISE, and the Rivers et al study. Second, the mortality
rate was lower than anticipated (27% vs 40%). This leaves the study underpowered
to detect a smaller treatment effect and may make the findings less applicable to
settings with higher mortality rates. Third, it is unclear just how different current
"usual care" is from EGDT. One-half of patients in the usual care group received a
central venous catheter and nearly two-thirds received an arterial catheter with
MAP monitoring, and at 6 hours and 72 hours CVP and MAP were similar. The
notable differences were ScvO2 monitoring and the concomitant protocol-driven
administration of dobutamine and red blood cells in response to low ScvO2 in the
EGDT arm, which seemed to yield no positive benefit, suggesting no role for
the routine use of ScvO2 monitoring and dobutamine in early sepsis management. It
could be argued that the lack of treatment effect in all three recent trials reflects in
part the incorporation into "usual care" of EGDT-inspired "Surviving Sepsis
Campaign" goals and the emphasis on early recognition of sepsis, early IV fluid
resuscitation, and early empiric antibiotic therapy.
Link out Via UTSW
7. Page | 7
A Randomized Trial of Icatibant in ACE-Inhibitor-Induced
Angioedema
Dr. James Galloway reviewing Bas M, et al. N Engl J Med. 2015;372(5):418-25.
Summary: There is growing information that Icatibant, a bradykinin B2 receptor
antagonist might be of therapeutic benefit in ACEI induced angioedema, but there is
limited data so far on its clinical significance.
Commentary:
ACE-inhibitors are responsible for one third of cases of angioedema of the upper
aerodigestive tract. The mechanism is believed to be bradykinin-mediated, but at
present there is no FDA approved, mechanistically-guided intervention for this
condition. This is a small, multicenter, double-blind, double-dummy, randomized
phase 2 trial assessing the efficacy and safety of a selective bradykinin B2 receptor
antagonist (icatibant 30 mg subcutaneous injection) compared to standard therapy
(IV prednisolone 500 mg plus antihistamine clemastine 2 mg) in the treatment of
ACE inhibitor-induced angioedema limited to the upper aerodigestive tract.
32 patients were screened and 27 patients were included in the analysis. Patients
were randomized within 10 hours of symptom onset in variable block sizes in a 1:1
ratio to ensure equal group sizes. There were no statistically significant differences
in baseline patient characteristics. The study had >90% power using two-sided
significance testing. No patients discontinued the study owing to adverse events;
however, 4 patients, all from the control group, were lost to follow up at day 14,
casting doubt on the validity of the safety analysis, although likely not affecting the
immediate efficacy outcomes.
A per protocol analysis was conducted, reflecting efficacy under optimal therapeutic
conditions. No patients in the experimental group failed treatment. Three patients in
the control group failed standard therapy at 6 hours and received "rescue therapy"
with the study agent and 500mg IV prednisolone; one of them required a
tracheotomy; these 3 patients were arbitrarily assigned the maximum recorded
time to complete resolution of edema (61.2 hours), which exaggerated the
difference in primary endpoint between the two groups.
The primary efficacy end point was time to complete resolution of edema, which
was evaluated using a composite of 3 scores: patient-assessed dyspnea, blinded
investigator-assessed dyspnea, and blinded investigator-assessed edema on
physical exam or endoscopy. The median time to complete resolution of edema was
8.0 hours with icatibant (IQR 3.0-16.0 hours) as compared with 27.1 hours (IQR
20.3-48.0 hours) with standard therapy (P=0.002). Among the secondary endpoints,
8. Page | 8
the median time to the onset of symptoms relief was significantly shorter with
icatibant vs standard therapy (2.0 hours vs 11.7 hours, P=0.03) when measured by
investigator assessed symptom scores; however, there was no difference in the
more meaningful measure of the patients' own assessments of their dyspnea. The
study was partly funded by the manufacturer.
In conclusion, this small phase 2 trial provides support for the efficacy of a selective
bradykinin B2 receptor antagonist in the early management of ACE inhibitor-
induced angioedema, although there were some methodological issues that likely
exaggerated the positive effect, and patient-centered outcomes were less robust.
Icatibant may shorten the duration of edema as compared with glucocorticoids plus
antihistamines under optimal therapeutic conditions, but it is unclear whether this
will translate in phase 3 studies into decreased intubations, ICU admissions, and
long-term complications.
10. Page | 10
Nephrology
High-Sensitivity Troponin T and N-Terminal Pro-B-Type
Natriuretic Peptide (NT-proBNP) and Risk of Incident Heart Failure
in Patients with CKD: The Chronic Renal Insufficiency Cohort
(CRIC) Study.
Dr. Natalia Rocha reviewing Bansal N, et al. JASN 2015; 26:946-956
Summary: The use of high sensitivity Troponin T and NT-proBNP even in CKD
patients is still a strong predictor of the incidence of heart failure.
Commentary: The use of high sensitivity troponin T (hsTnT) and NT-proBNP as
predictors of heart failure in CKD patients has been limited due to concerns that
elevations might simply be a reflection of decrease biomarker clearance from
decreased GFR. In this prospective cohort analysis, the authors studied 3483
patients with mild to severe CKD enrolled in the Chronic Renal Insuficiency Cohort
(CRIC) study with no heart failure. They examined the association between baseline
hsTnT and NT-proBNP and subsequent incident HF. The authors concluded that
even after adjusting for a vast range of cardiovascular risk factor such as older age,
sex, race, higher BP, diabetes and lower rejection fraction, hsTnT and NT-proBNP
were both strong predictors of incident heart failure in patients with mild to
moderate CKD and may represent subclinical injury that can ultimately progress to
HF.
Link Out Via UTW
11. Page | 11
Preoperative renin–angiotensin system inhibitors use linked to
reduced acute kidney injury: a systematic review and meta-
analysis
Dr. Natalia Rocha reviewing Cheungpasitporn W, et al. Nephrol. Dial.
Transplant. 2015; doi: 10.1093/ndt/gfv023
Summary: The meta-analysis suggesting negative outcomes with the use of RAS
inhibitors pre-operatively may have been limited by confounding factors. Limiting
these confounding factors by the use of propensity scores has actually shown a
decrease in AKI postop with the use of preoperative RAS inhibitors.
Commentary: Acute kidney injury (AKI) is one of the most frequent postoperative
complications and it is linked to higher hospital mortality. A previous meta-analysis
of observational studies showed that the preoperative use of a renin-angiotensin
system (RAS) inhibitor was associated with increased incidence of AKI
postoperatively and for this reason, discontinuation of RAS inhibitors prior to
surgery has been proposed as a preventative measure for postoperative AKI. The
study of Cheungpasitporn et al suggests that the previous meta-analysis might have
been limited by the effect of confounders such as the fact that patients on RAS
inhibitors are usually the ones with heart failure, hypertension and diabetes, which
are all risk factors for AKI. The authors found that by utilizing propensity scores,
which reduced confounding effect, there was a significant association between
preoperative RAS inhibitor use and lower incidence of AKI. The association was
stronger when RAS inhibitor was used for > 2 weeks prior to surgery. The
physiological explanation for this protective effect is that reducing RAS response to
renal ischemia during surgery leads to decrease in systemic vascular resistance and
improve renal plasma flow.
Link Out Via UTSW
12. Page | 12
Cardiology
Which drug should we use for stroke prevention in atrial
fibrillation?
Dr. Douglas Darden reviewing Lau, Yee C.; Lip, Gregory Y.H. Current Opinion in
Cardiology. 2014 July 29 (4): 293-300.
Summary: This article reviews the latest evidence and development of new oral
anticoagulants for the prevention of ischemic stroke, as well as bleeding risk
assessment, mitigation and management.
Commentary: Decision-making for stroke prevention has evolved towards the
initial identification of 'low-risk' patients who do not need any antithrombotic
therapy. Subsequent to this step, patients with at least 1 stroke risk factor can be
offered effective stroke prevention, which is OAC. There is increased morbidity and
mortality amongst warfarin users, if time in therapeutic range is poor. New oral
anticoagulants (such as dabigatran, rivaroxaban, apixaban and edoxaban) offer
relative efficacy, safety and convenience compared to warfarin, in relation to stroke
prevention in atrial fibrillation. Bleeding risk can be assessed by HAS-BLED score,
whereas the new SAMe-TT2R2 score can predict the patient's suitability for vitamin
K antagonists. It is well-known that vitamin K antagonists (VKAs), such as warfarin,
is highly effective and has been shown to reduce stroke risk by 64% and all-cause
mortality by up to 26% in atrial fibrillation. However, the use of VKA is complicated
by its potential interactions with food and medications, genetic polymorphisms
conferring differing susceptibilities, as well as the potential for major hemorrhage.
And of course, the effectiveness of VKA treatment depends on the time spent in
therapeutic range, with maximum benefit achieved if time spent in therapeutic
range exceeds 70%.
The limitations of VKA have led to the development of NOACs, ‘novel’ or ‘non-VKA
oral anticoagulants’. Through reversible inhibition of thrombin by dabigatran or
Factor Xa by rivaroxaban, apixaban or edoxaban, the NOACs exhibit a predictable
pharmacology that allow for fixed dosing that makes monitoring unnecessary (see
table 1 for the major RCTs).
Dabigitran was studied in the RE-LY trial, where it was found to be superior to
warfarin for prevention of both ischemic stroke and systemic thromboembolism,
with an annual event of 1.11% in the 150 mg group and 1.53% in the 110 mg group
against warfarin-treated patients at 1.69% (P < 0.001). Dabigatran was also non-
inferior to warfarin for major bleeding with annual event rates of 3.11% in the 150
mg group vs. 2.71% in the 110 mg group vs. 3.36% in the warfarin-control group. It
was also superior to warfarin in reducing intracranial hemorrhage by more than
half.
13. Page | 13
Rivaroxaban was studied in the ROCKET-AF trial and showed to be non-inferior
compared to warfarin the prevention of ischemic stroke. Apixaban, on the other
hand, was showed to be superior to warfarin in the ARISTOTLE trial, with the
annual event rate of 1.27% in the apixaban group vs. 1.6% in the warfarin group.
One of the drawbacks currently with the NOACs is that there is no antidote. In
assessing the stroke and bleeding risk for patients, we all know to use the CHA2DS2-
VASc score and HASBLED score. To note, a high HAS-BLED score should identify
potential risk factors that can be treated, rather than withhold anticoagulation
(table 2). To aid in deciding between VKA and NOACs, the SAMe-TT2R2 score (table
3) has been created to identify those who will do well on VKA (score 0-1).
Lastly, as there is insufficient on NOACs in ESRD and prosthetic heart valves, VKA is
still the preferred option.
Table 1: Randomized controlled trials for NOACs in Atrial Fibrillation
14. Page | 14
Table 2: HAS BLED scoring system
Table 3:
SAMe-TT2R2 score
Link Out Via UTSW
15. Page | 15
EKG CHALLENGE:
Contributed by Dr. Jeanney Lew
A 57 year-old male with T2DM, HTN, and current tobacco use presents to the ED with a
3-day history of severe intermittent chest pain, which he describes as 7/10 “crushing”
substernal pressure. These episodes have been associated with shortness of breath and
diaphoresis, seemingly triggered by exertion, resolving after 10 minutes of rest. This
morning the pain felt so severe that he “took a couple aspirin and called 911.” Upon
arrival to the ED, his chest pain had resolved – He was resting comfortably, not in
distress. His vitals: T 37 C, P 90, BP 142/88, RR 16, SpO2 99% on RA. Initial troponin T
was 0.01 and EKG performed at this time (EKG 1) was significant for biphasic T waves in
leads V2 and V3 and inverted T waves in leads V4 and V5.
EKG 1
After 2 hours of sitting in the ED, patient suddenly develops severe 10/10 crushing
substernal pain, SOB, and palpitations. He appears diaphoretic and in significant
distress. Repeat troponin T was drawn – measured 0.24 and STAT EKG revealed the
following:
EKG 2
At this point, Cardiology was consulted and another STAT EKG showed the following
changes:
EKG 3
16. Page | 16
QUESTIONS:
What is this patient’s diagnosis?
What is the significance of his EKG findings on initial presentation?
What is the appropriate management?
DISCUSSION:
This patient was taken to the cath lab for emergent PCI – found to have
occlusion of the proximal LAD for which he received one drug-eluting stent.
His clinical presentation is classic for Wellens’ Syndrome (AKA: LAD Coronary
T wave syndrome / “widow-maker”) – a combination of characteristic EKG
changes in a patient with intermittent chest pain. It is seen in patients with critical
stenosis of the proximal LAD. The dynamic EKG changes (T wave changes) represent
transient occlusion and re-perfusion of the LAD. Without intervention, 75% of these
patients will progress to acute anterior wall myocardial infarction within one week [1].
Wellens’ Syndrome Criteria [2]:
History of intermittent chest pain
Normal / slightly elevated cardiac markers
The following EKG findings (during pain-free state):
o Biphasic or deeply inverted T waves in V2 to V3 (+/- other
precordial leads)
o No / minimal ST segment elevation (<1 mm)
o No precordial Q waves
o Preserved precordial R wave progression
EKG 1 – WELLENS’ WAVES: biphasic T waves in leads V2 and V3 and deep, inverted T
waves in leads V4 and V5
LAD is patent, but with high-grade stenosis. Patient is at risk of LAD occlusion
and anterior MI.
17. Page | 17
EKG 2 – “PSEUDO-NORMALIZATION” of the T waves: upright “hyperacute T waves” in
anterior leads
Occlusion of the LAD and early transmural MI
18. Page | 18
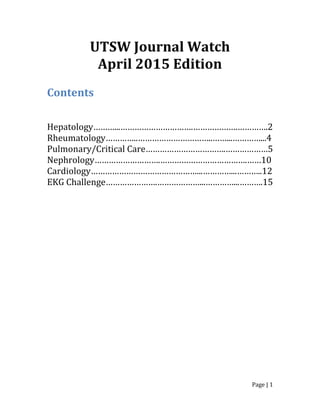
EKG 3 - ACUTE ANTERIOR ST-ELEVATION MYOCARDIAL INFARCTION
ST segment elevation in anterior leads V1 to V5
Reciprocal changes in inferior leads (II, III, aVF)
KEY POINTS:
Wellens’ waves are bipashic or deeply inverted T waves in anterior leads (esp V2,
V3)
Wellens’ syndrome = Wellens’ waves in a patient with history of intermittent
chest pain
o During pain-free intervals; troponins are normal or minimally elevated
o LAD is patent, but at high risk of occlusion, resulting in acute anterior wall
MI
o This is an indication for urgent cardiac cath
“Pseudo-normalization” (upright, hyperacute T waves) = occlusion of the LAD
o Represents early phase of myocardial infarction
o Accompanied by chest pain, rising cardiac enzymes
REFERENCES:
1. Mead, N.E. and K.P. O'Keefe, Wellen's syndrome: An ominous EKG pattern. J
Emerg Trauma Shock, 2009. 2(3): p. 206-8.
2. Yusuf Muharam, M., R. Ahmad, and M. Harmy, The ' widow maker':
Electrocardiogram features that should not be missed. Malays Fam Physician,
2013. 8(1): p. 45-7.