Download to read offline

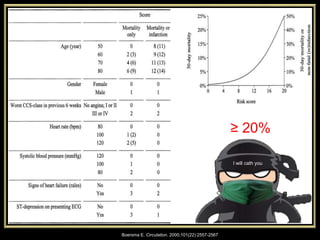

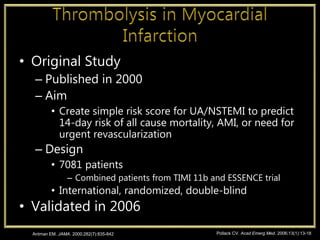
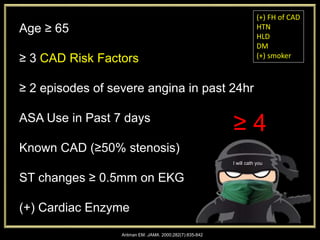
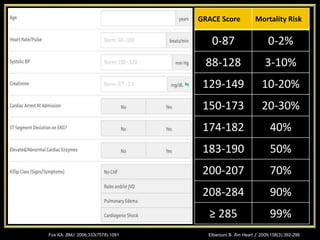

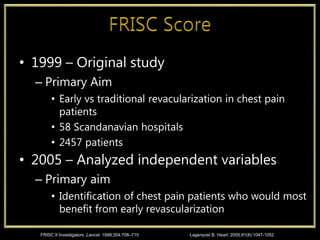
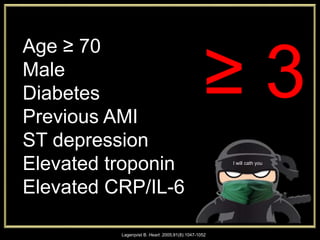

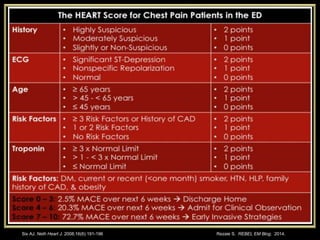
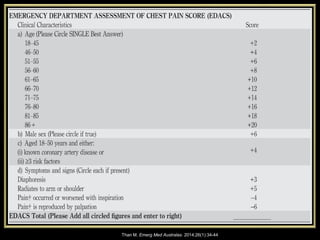


Kristopher Maday, MS, PA-C is the Program Director and Associate Professor at the University of Tennessee Health Science Center Physician Assistant Program. He provided a summary of several risk scores used to risk stratify patients presenting with chest pain including the PURSUIT, TIMI, GRACE, FRISC, HEART, and EDACS scores. Several of these scores such as GRACE and TIMI were developed and validated in large international randomized controlled trials to predict short and long term risks of death and myocardial infarction. The FRISC trial examined the benefit of early revascularization in unstable coronary syndrome patients. The EDACS score was derived and validated in two hospital studies to predict low risk in an accelerated







































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















