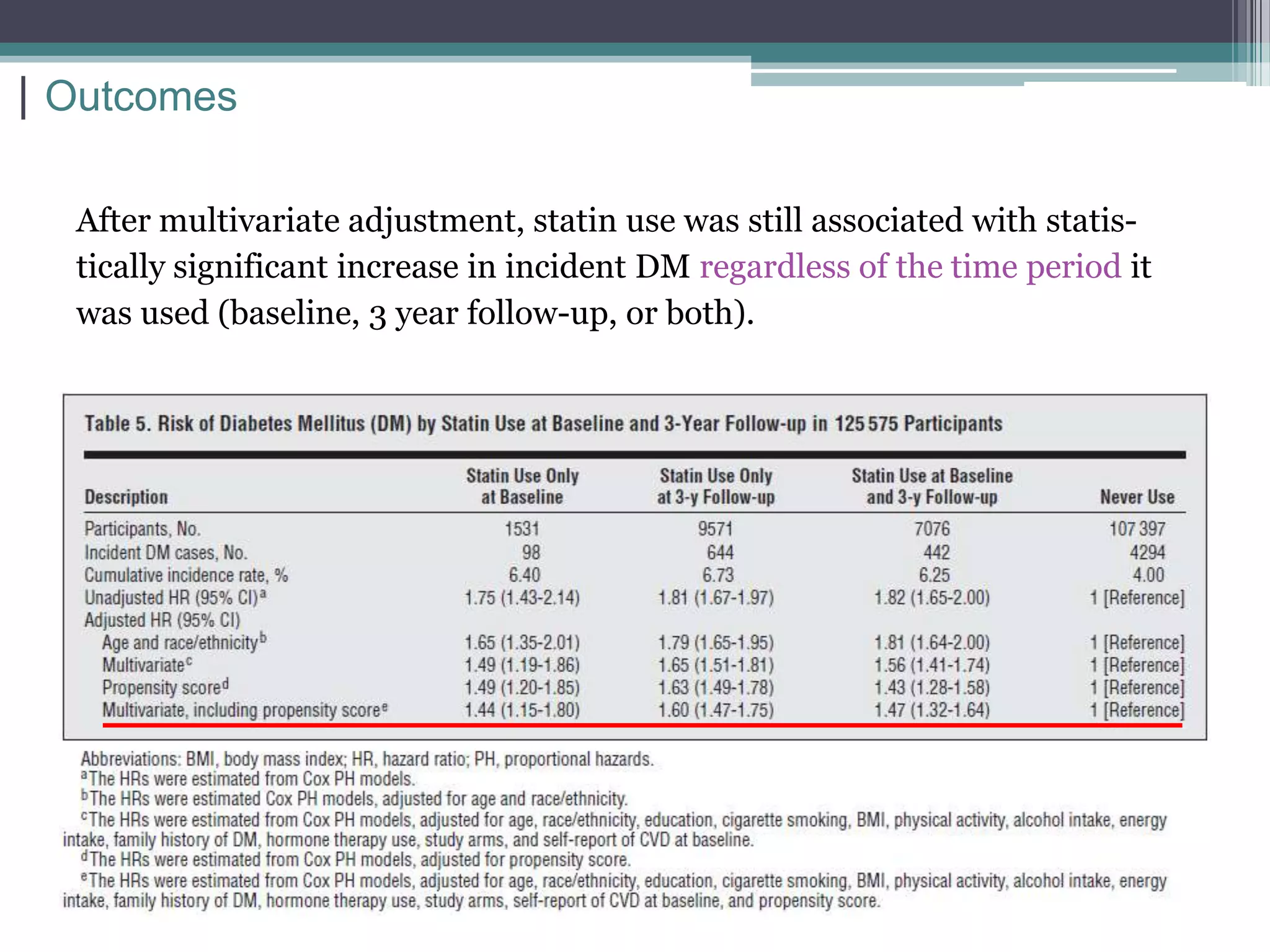
Statin use was associated with a statistically significant increased risk of developing diabetes in postmenopausal women according to a study using data from the Women's Health Initiative. The risk was found across all subgroups tested and persisted even after adjusting for potential confounding factors. However, the study did not prove causation and a subset analysis using fasting glucose did not replicate the increased risk finding. The authors conclude statins have cardiovascular benefits but more research is needed to establish if they causally increase diabetes risk.