Download to read offline

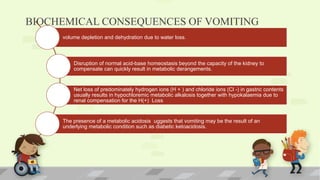

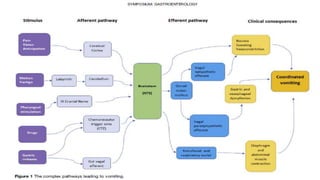
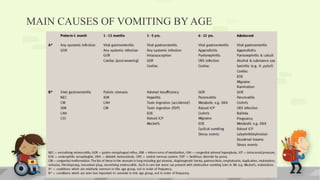


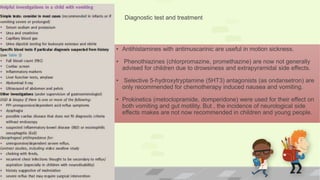

This document discusses the approach to evaluating and treating a vomiting child. It begins by outlining the complex physiology involved in vomiting and how different conditions can cause vomiting depending on a child's age. It then discusses the biochemical consequences of vomiting like dehydration. The mechanisms of vomiting are explained involving central and enteric nervous systems. Main causes of vomiting are discussed for different age groups. Key questions to ask the patient are mentioned. Finally, the document discusses some medication options for treating vomiting and emphasizes the importance of diagnostic testing.


































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
