Download to read offline
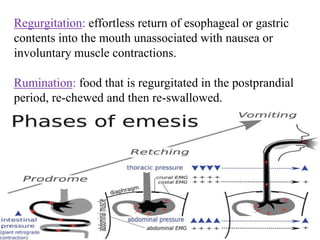
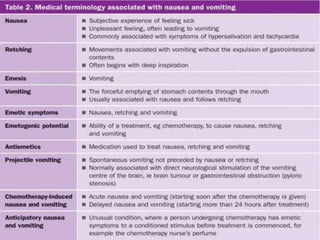
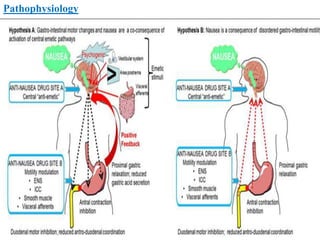
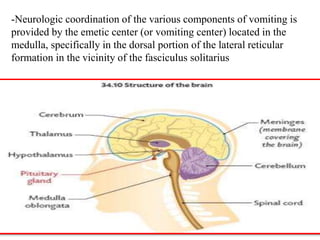
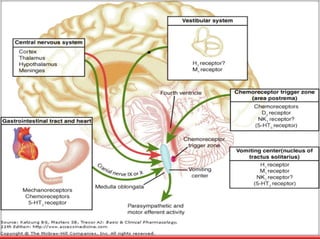

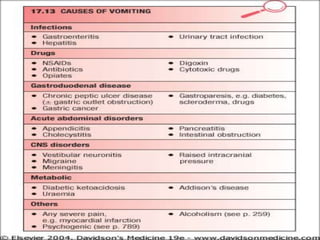
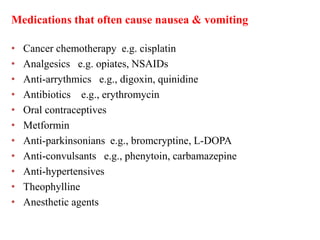
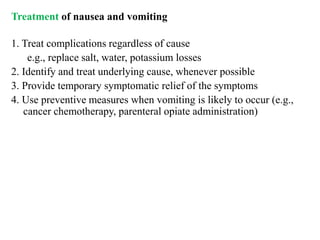
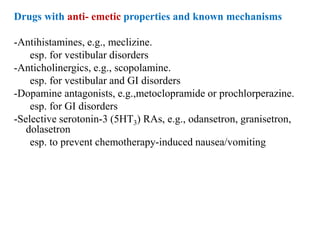


This document discusses vomiting and anti-emetic drugs. It defines different types of vomiting and regurgitation. It describes the pathophysiology of vomiting which involves the vomiting center in the brainstem coordinating stomach contractions and protective reflexes. Common causes of vomiting are then outlined including abdominal issues, infections, metabolic disorders and nervous system problems. Finally, it lists several classes of anti-emetic drugs like antihistamines, anticholinergics, and 5HT3 receptor antagonists; and describes how they work to treat nausea and vomiting.



































































