Download to read offline

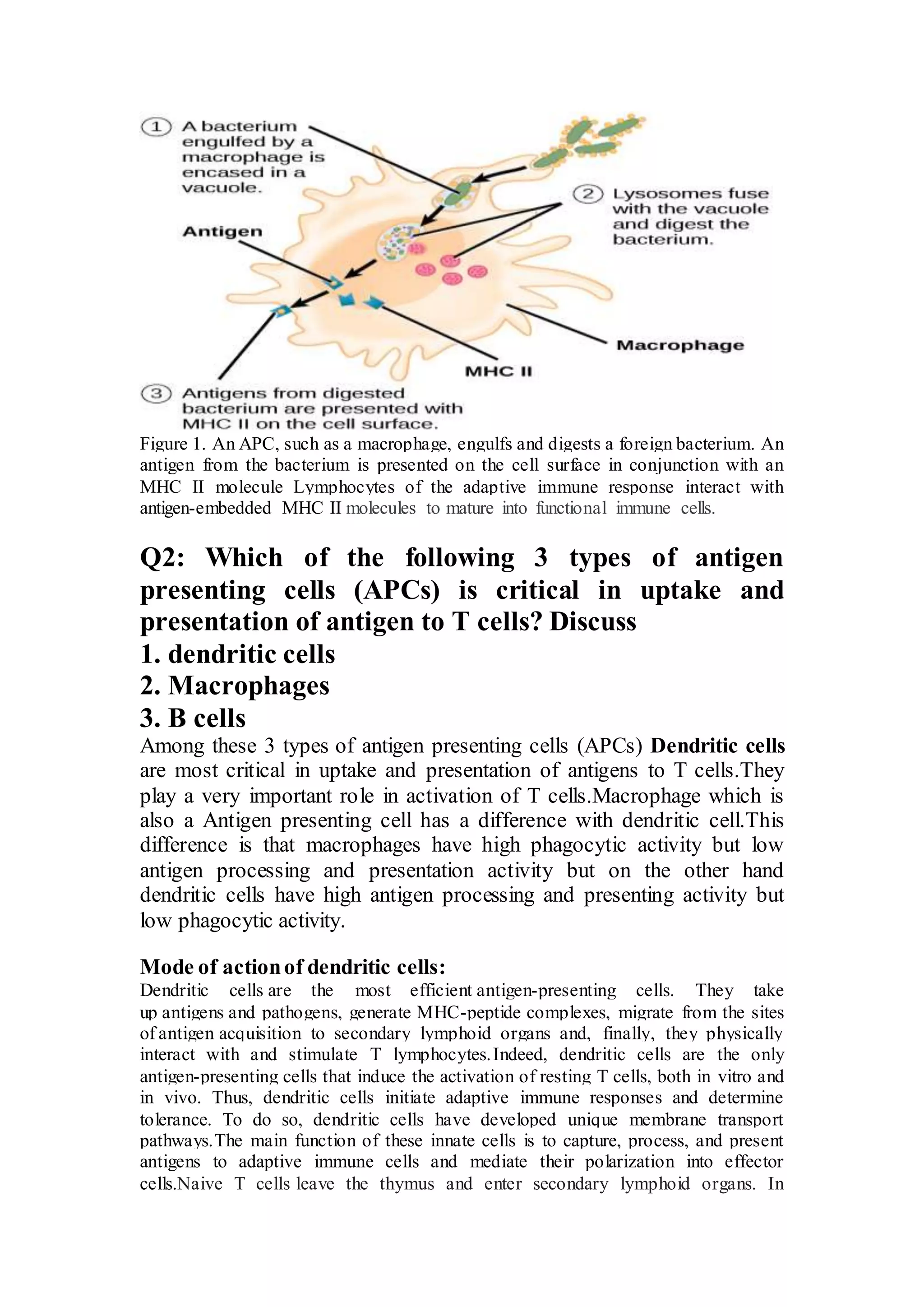


The document discusses the functions of antigen-presenting cells (APCs), specifically focusing on dendritic cells, macrophages, and B cells in their roles in the immune response. It details how macrophages excel in degradation and presentation of particulate antigens, while dendritic cells are critical for uptake and activation of T cells. Additionally, it explains the mechanisms of antigen processing and presentation by these cells, illustrating their importance in both innate and adaptive immunity.



































































