




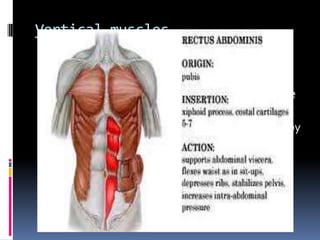
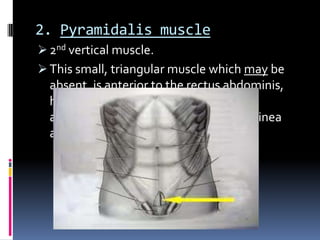
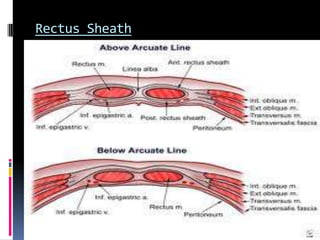
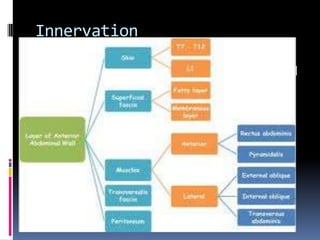
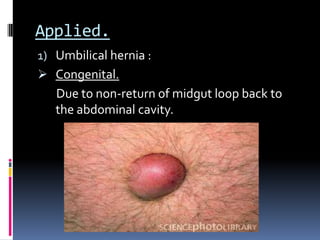






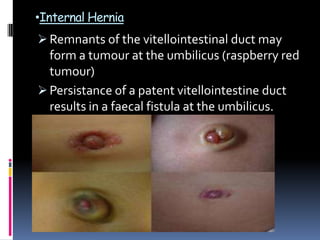
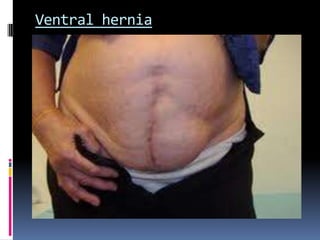




The document discusses the anatomy of the anterolateral abdominal wall. It describes the five muscles that make up the anterolateral wall - the external oblique, internal oblique, transversus abdominis, rectus abdominis, and pyramidalis. It details the structure, function and innervation of these muscles. The document also discusses the blood supply, lymphatic drainage and applied clinical considerations like different types of hernias related to weaknesses in the abdominal wall.



































































