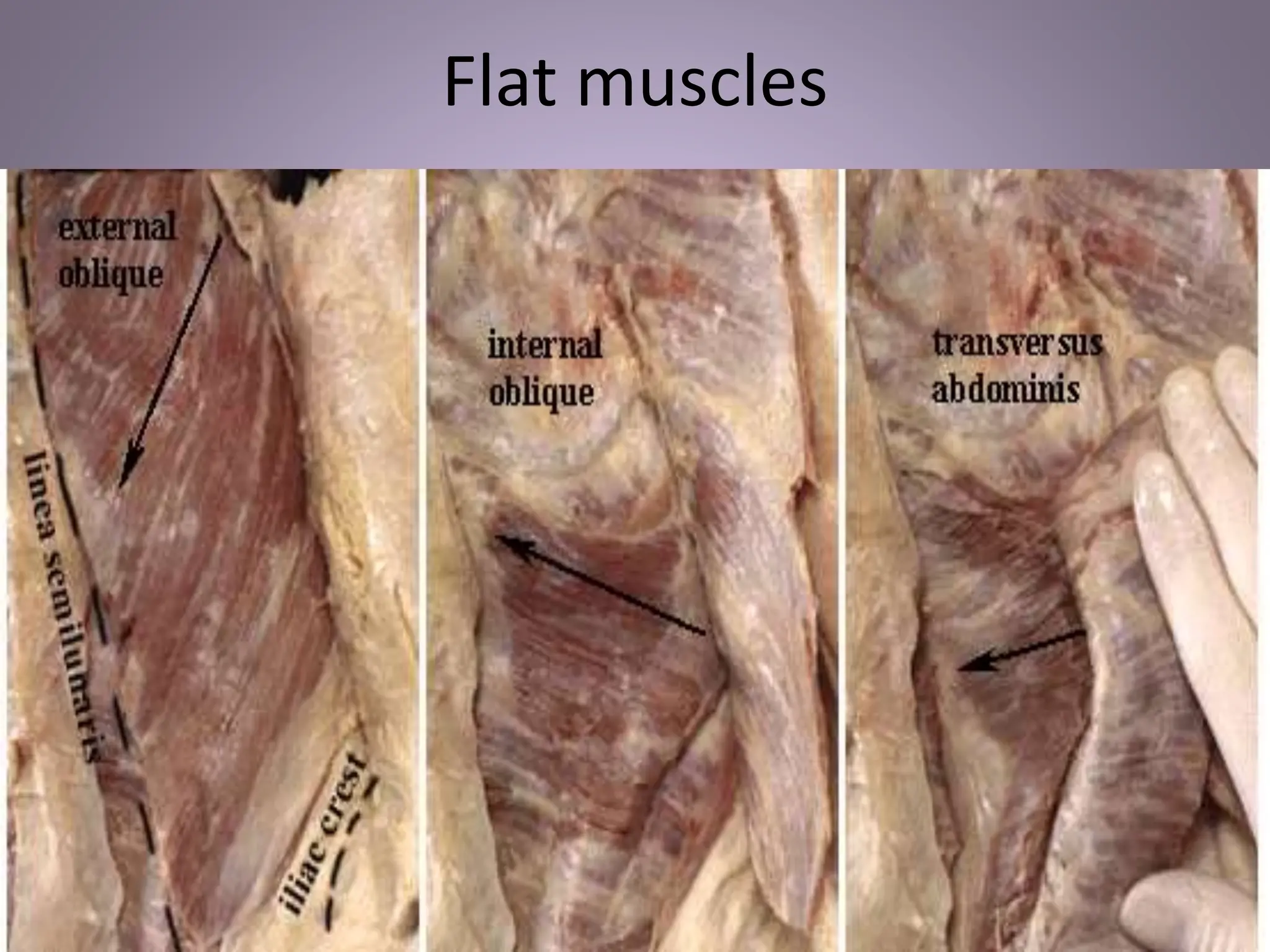
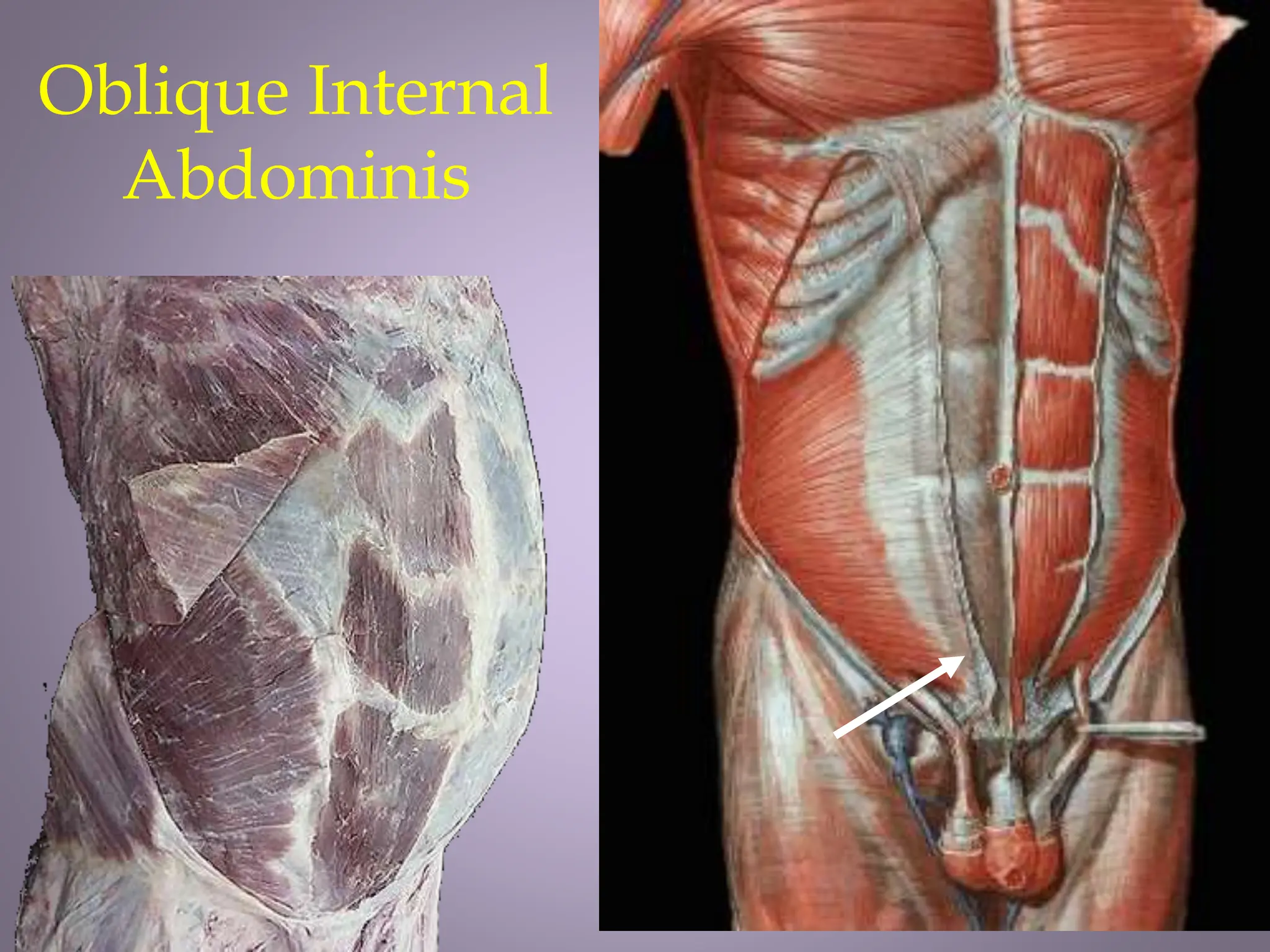
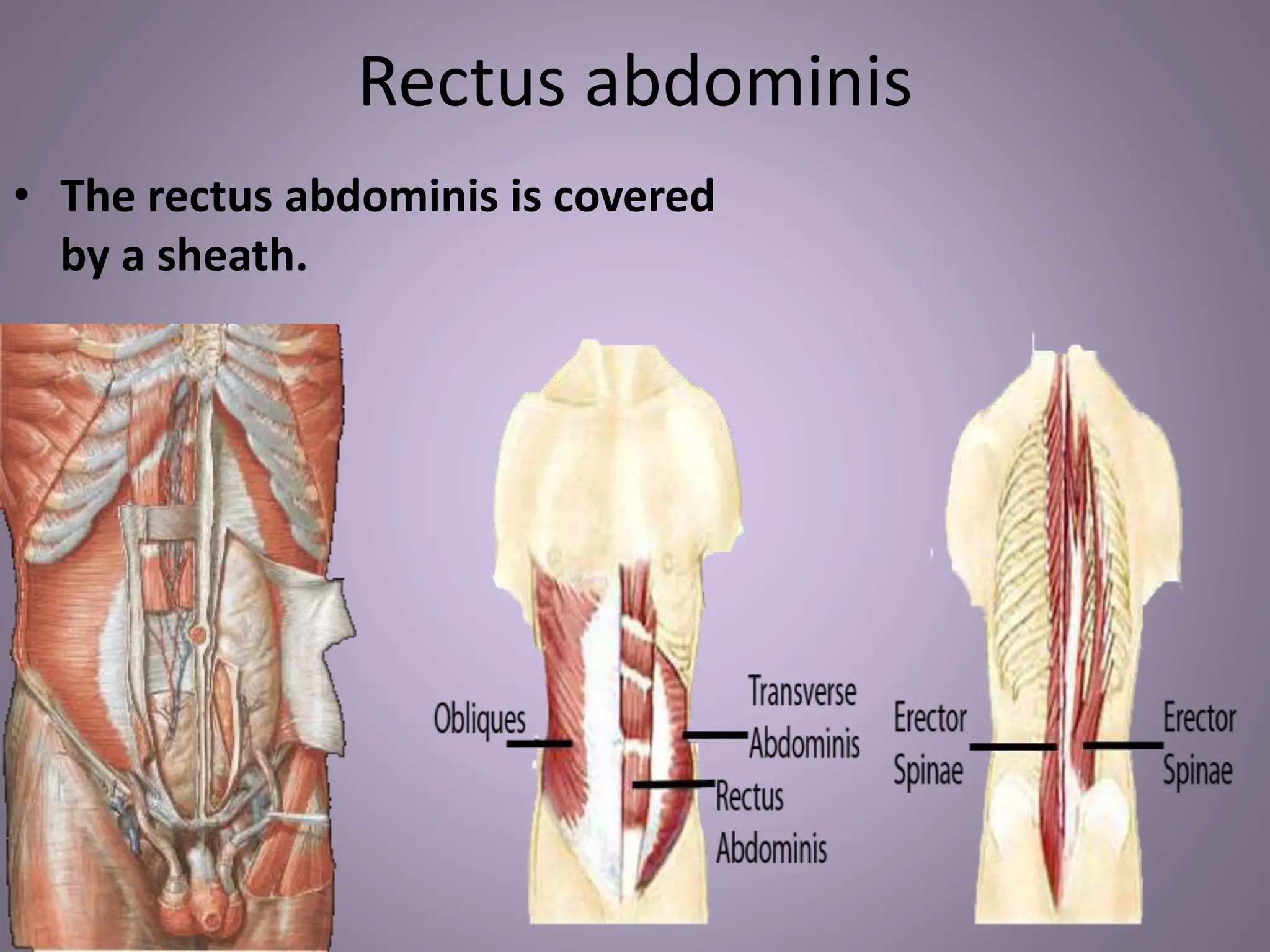
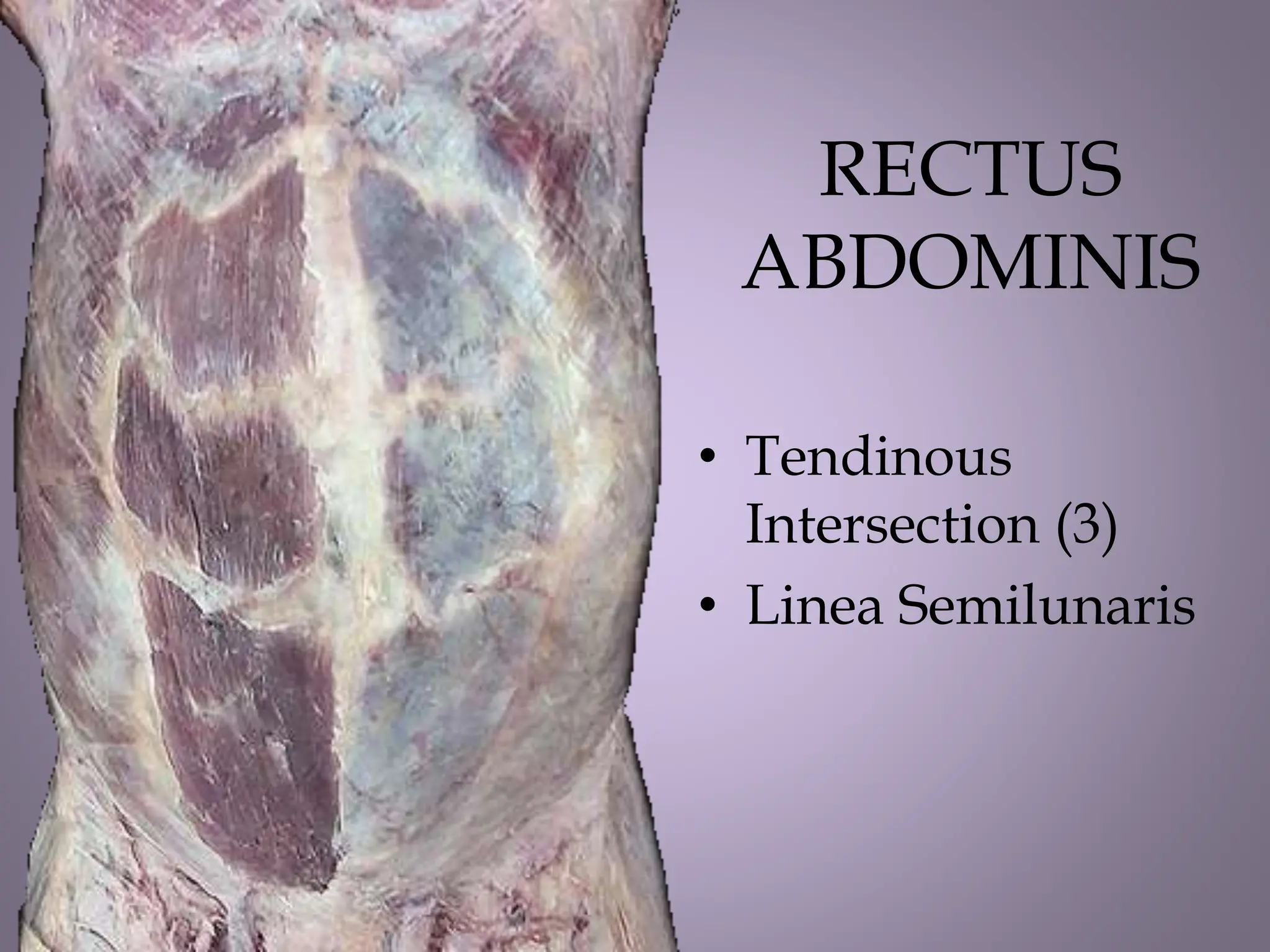
The document provides a comprehensive overview of the anatomy of the anterior abdomen and peritoneum, detailing the organization of the abdominal wall, muscle layers, blood supply, and innervation. It discusses the quadrants and regions of the abdomen, the significance of linea alba, and the structure and function of the rectus sheath. Additionally, it covers important clinical considerations regarding surgical incisions, lymphatic drainage, and the inguinal canal's anatomy and function.