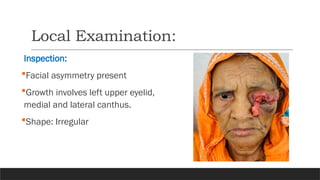
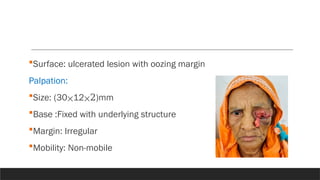
Mrs. Rahima Begum, an 80-year-old female from Dhaka, presented with a rapidly growing, ulcerated lesion on her left upper eyelid, eventually diagnosed as sebaceous gland carcinoma, alongside age-related cataract in her right eye. She has been managing diabetes and hypertension without prior medical intervention for her eyelid growth. A plan for management includes biopsy, chemotherapy, and cataract extraction.