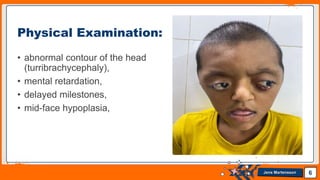
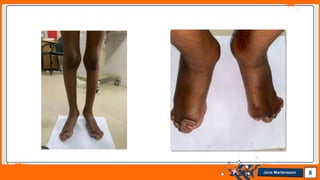
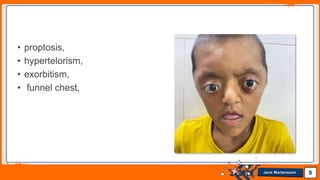
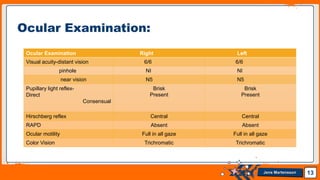
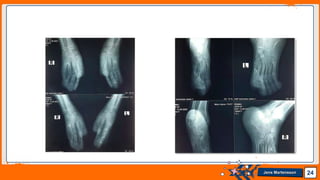
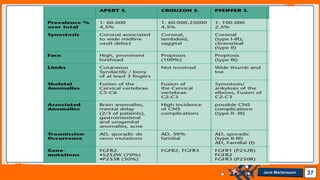
Master Jikir Hossain, a 9-year-old male from Nator, Bangladesh, presented with proptosis of both eyes, swelling of the left eyelid, and incomplete eyelid closure for 7 months. Physical examination found syndactyly of both hands and feet, abnormal head shape, and mental retardation. Based on these findings and a family history of nonconsanguineous parents, a provisional diagnosis of Apert syndrome was made. Further examinations including CT scan of the brain confirmed features consistent with Apert syndrome, which is a genetic disorder caused by mutations in the FGFR2 gene. The patient's management will involve surgery and input from ophthalmology and neurosurgery.