Downloaded 17 times







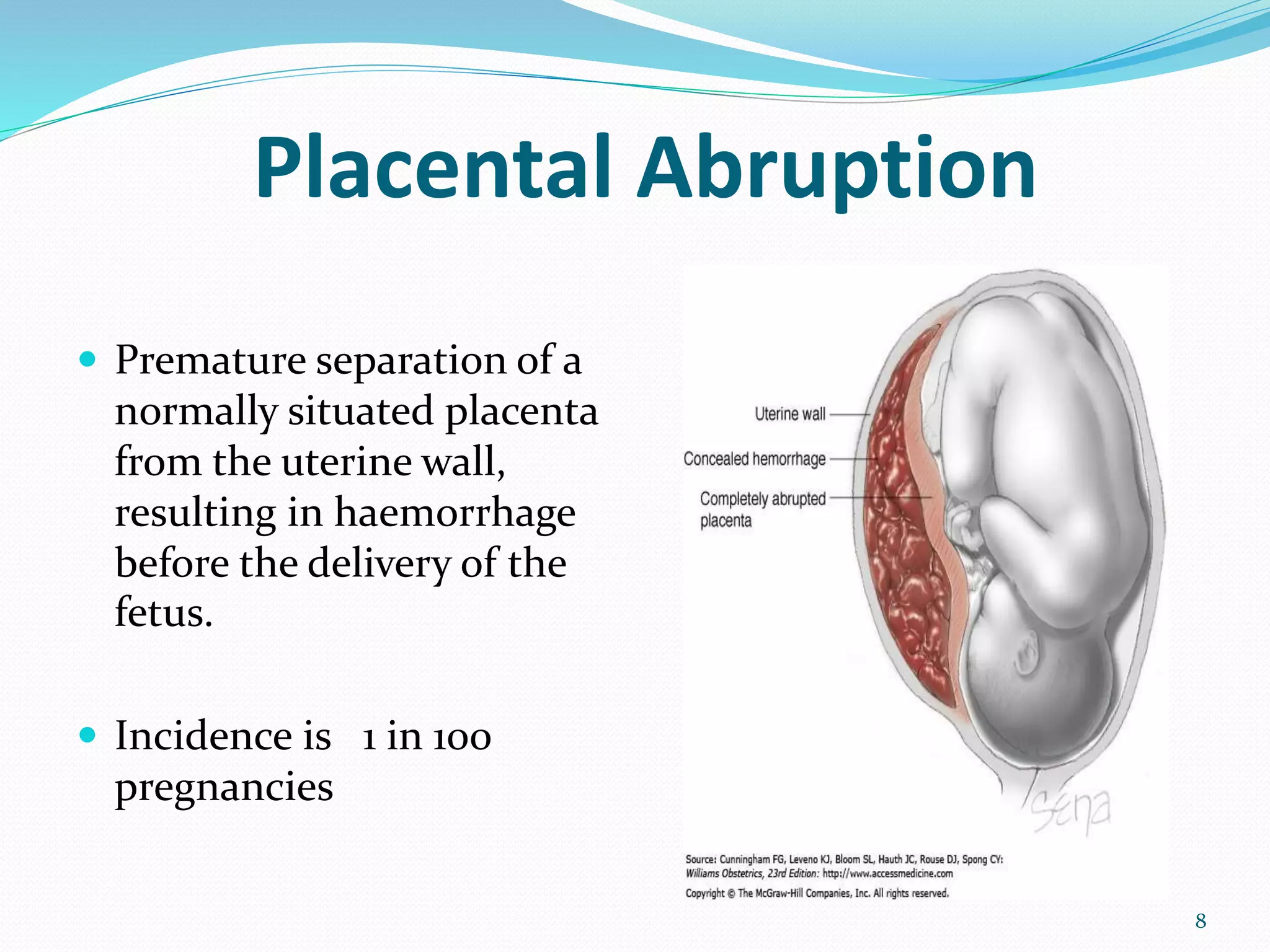
































This document discusses antepartum hemorrhage (APH), specifically focusing on placental abruption and placenta previa. It defines APH as bleeding from or into the genital tract occurring after 24 weeks of gestation and prior to birth. Placental abruption is defined as premature separation of the placenta from the uterine wall, occurring in about 1% of pregnancies. Risk factors include increased age, previous abruption, hypertension, and trauma. Placenta previa is implantation of the placenta in the lower uterine segment, occurring in about 4-5 per 1,000 pregnancies. Risk factors include previous cesarean sections and multiparity. Both conditions require careful management to prevent

































![obstetric 1 antinatal care for midwifery].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604190707-264c2efa-thumbnail.jpg?width=640&height=640&fit=bounds)
![obstetric 2 lecture note for health].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604192427-51f7250b-thumbnail.jpg?width=640&height=640&fit=bounds)

![ANTEPARTUM HAEMORRHAGE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/antepartumhaemorrhageautosaved-230213084941-60834529-thumbnail.jpg?width=640&height=640&fit=bounds)






























