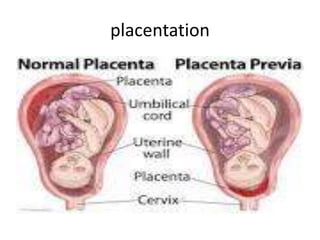
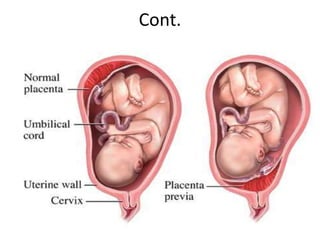
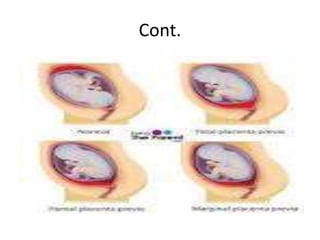
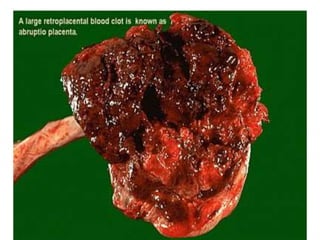
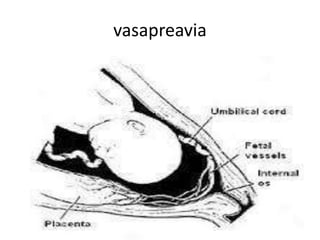
This document provides an overview of antepartum hemorrhage (APH), specifically focusing on placenta previa, abruption placentae, and vasa previa. It defines each condition, discusses causes, risk factors, clinical presentation, diagnosis, and management. Placenta previa is defined as implantation of the placenta in the lower uterine segment and is a leading cause of APH. Abruptio placentae is premature separation of a normally implanted placenta. Vasa previa occurs when fetal blood vessels cross the cervical opening. All three conditions can result in life-threatening bleeding and require careful monitoring and management to optimize maternal and fetal outcomes.


















![Breech presentation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/breechpresentationautosaved-211128120250-thumbnail.jpg?width=640&height=640&fit=bounds)





























![obstetric 1 antinatal care for midwifery].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604190707-264c2efa-thumbnail.jpg?width=640&height=640&fit=bounds)
![obstetric 2 lecture note for health].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/l-1bleedinginlatepregnancy1-240604192427-51f7250b-thumbnail.jpg?width=640&height=640&fit=bounds)



















![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
