Downloaded 1,011 times


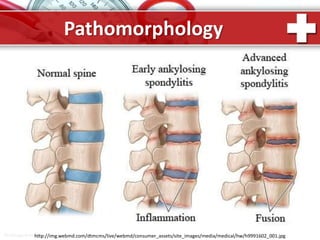
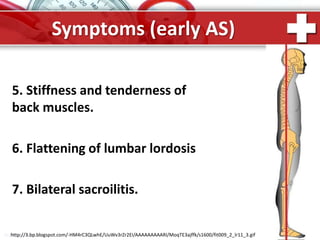
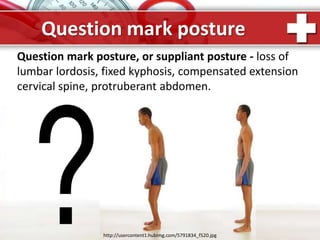
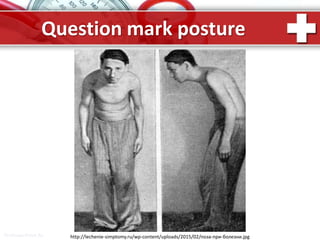

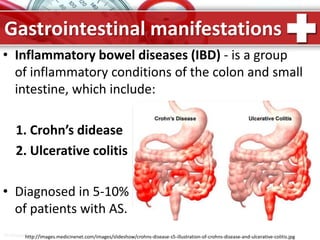









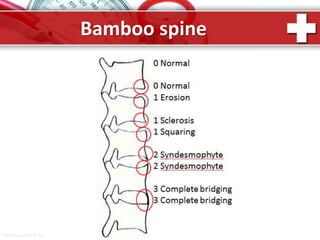
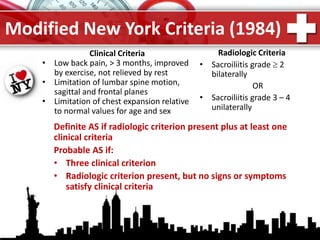
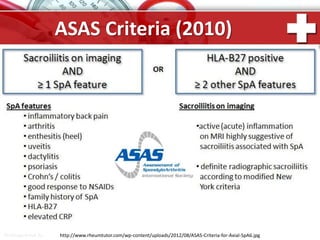

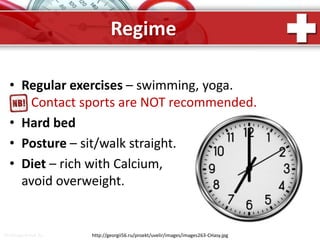


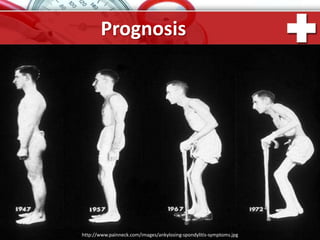


This document provides information about ankylosing spondylitis (AS), including its definition, symptoms, signs, and management. AS is a chronic inflammatory disease that mainly affects the spine and sacroiliac joints, causing stiffness, pain and fusion of the vertebrae. It has strong genetic associations with HLA-B27 antigen and may be triggered by bacterial infections. Symptoms often begin with lower back pain and stiffness that worsens with rest and improves with activity. Advanced cases can result in a fixed "question mark" posture as the spine becomes fused. The document discusses diagnostic criteria, extra-articular manifestations involving the eyes, heart, lungs and bowels, and treatment approaches for AS.




















































![ANKYLOSING_SPONDYLOSIS[1].pptx dr.harsh.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ankylosingspondylosis1-260112172605-e0b9270e-thumbnail.jpg?width=640&height=640&fit=bounds)























![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










