Download to read offline






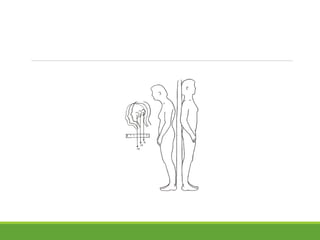


















- Ankylosing spondylitis is an inflammatory disorder that primarily affects the axial skeleton including the spine and sacroiliac joints. It has a strong association with the HLA-B27 gene. - The disease usually begins in young adults and presents as inflammatory back pain. Diagnosis requires radiographic evidence of sacroiliitis along with symptoms of back pain and stiffness. - While the exact cause is unknown, it is thought to be immune-mediated potentially triggered by intestinal bacteria in genetically susceptible individuals with HLA-B27. Tumor necrosis factor inhibitors can provide relief of symptoms.











































![ANKYLOSING_SPONDYLOSIS[1].pptx dr.harsh.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ankylosingspondylosis1-260112172605-e0b9270e-thumbnail.jpg?width=640&height=640&fit=bounds)























