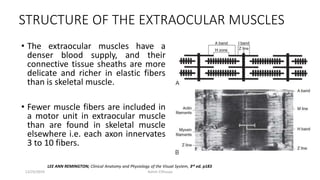
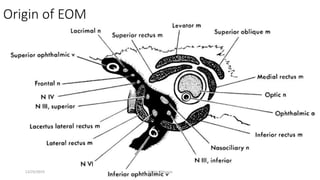
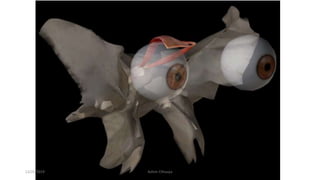
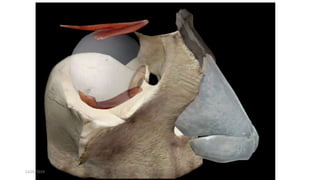
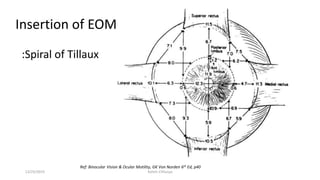
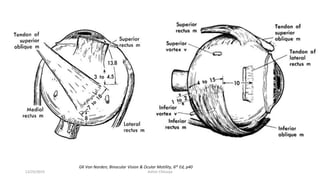
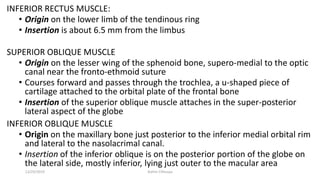
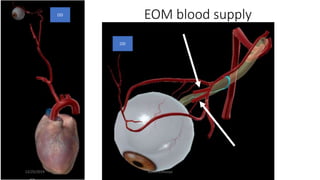
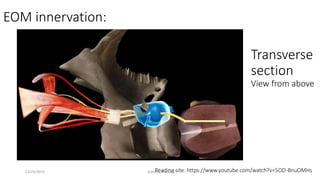

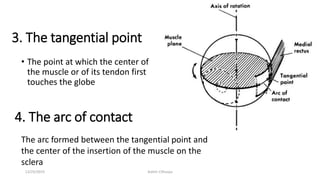
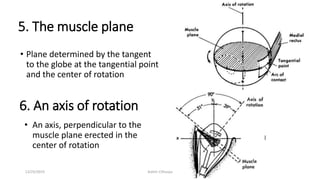
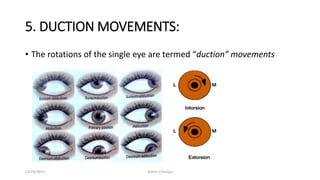
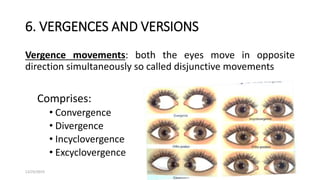

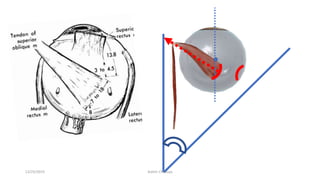
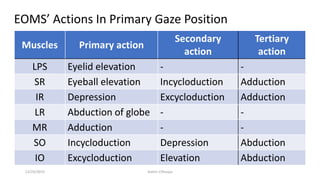
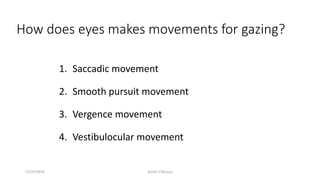
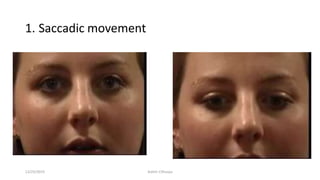
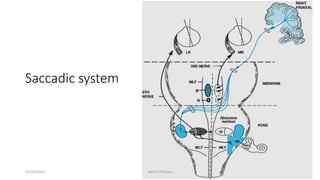
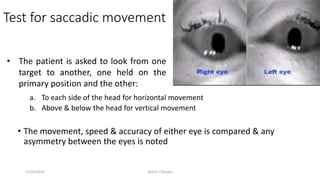
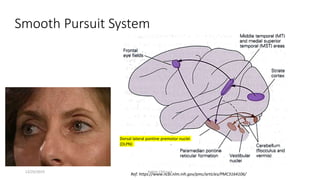



The document discusses the anatomy and function of the extraocular muscles. It provides details on: 1) The origin and insertion points of the 6 extraocular muscles. The muscles originate at bony landmarks in the orbit and insert on the sclera at distances of 5.5-7.7mm from the limbus. 2) The innervation and blood supply of the extraocular muscles which allows for precise control of eye movements. 3) The types of eye movements including versions, vergences, saccades, smooth pursuit, and vestibulo-ocular reflex. Each type of movement involves different neural pathways and muscle coordination.


































































