Download to read offline

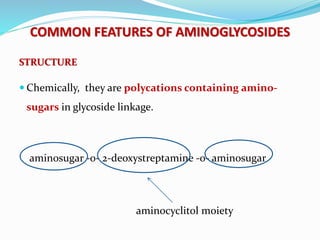
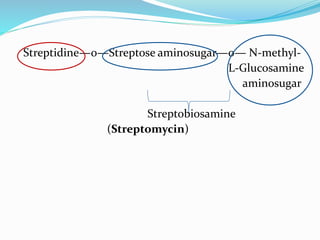
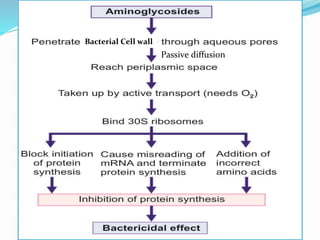
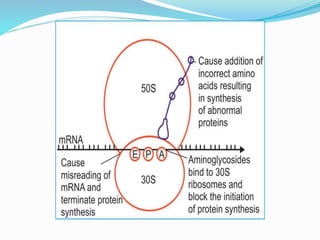
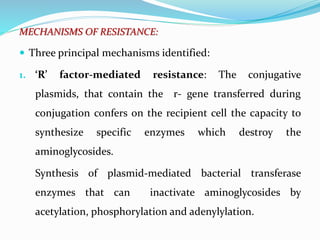
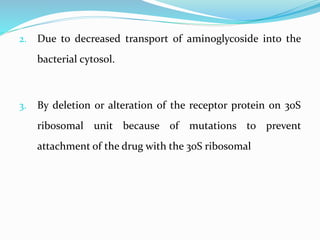
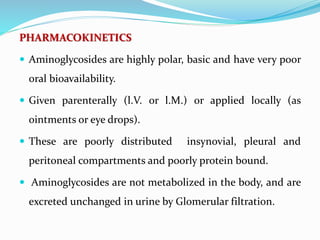
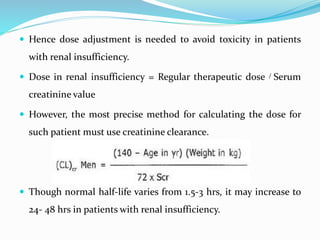

This document discusses aminoglycoside antibiotics. It begins by listing the key learning objectives which include explaining the mechanisms of action and resistance of aminoglycosides, describing different dosing regimens, monitoring therapy to avoid toxicity, and the unique features of individual drugs. It then covers the common structural features and characteristics of aminoglycosides, their mechanisms of action, and causes of resistance. The advantages and disadvantages of different dosing regimens are outlined. Signs of ototoxicity and nephrotoxicity are described along with monitoring therapy. Individual drugs like gentamicin, streptomycin, and amikacin are discussed in terms of their uses, doses, and spectra of activity.






















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)









