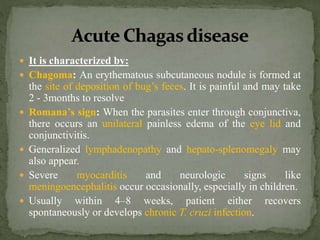
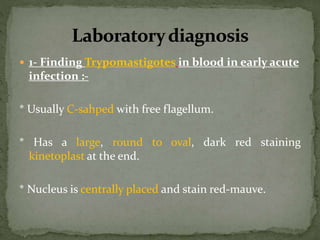
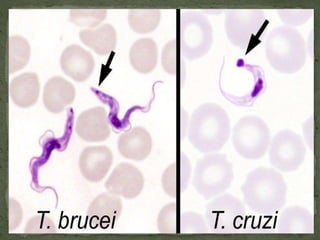
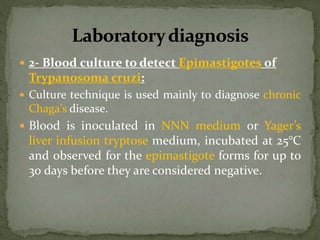
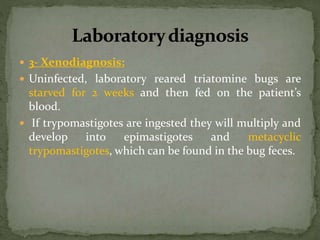
American trypanosomiasis, also known as Chagas disease, is caused by the parasite Trypanosoma cruzi. It is transmitted to humans through the feces of triatomine bugs and can also be spread through blood transfusions, organ transplants, and from mother to fetus. The parasite infects tissues like the heart, digestive system, and nervous system. In the acute phase, symptoms may include swelling at the site of infection and eye swelling. In the chronic phase years later, cardiac or gastrointestinal complications can occur. Diagnosis involves microscopic examination of blood or culture to detect parasite forms, or serological tests.
























![Trypanosoma [1]](https://cdn.slidesharecdn.com/ss_thumbnails/trypanosomaseminar1-170312074241-thumbnail.jpg?width=640&height=640&fit=bounds)















































