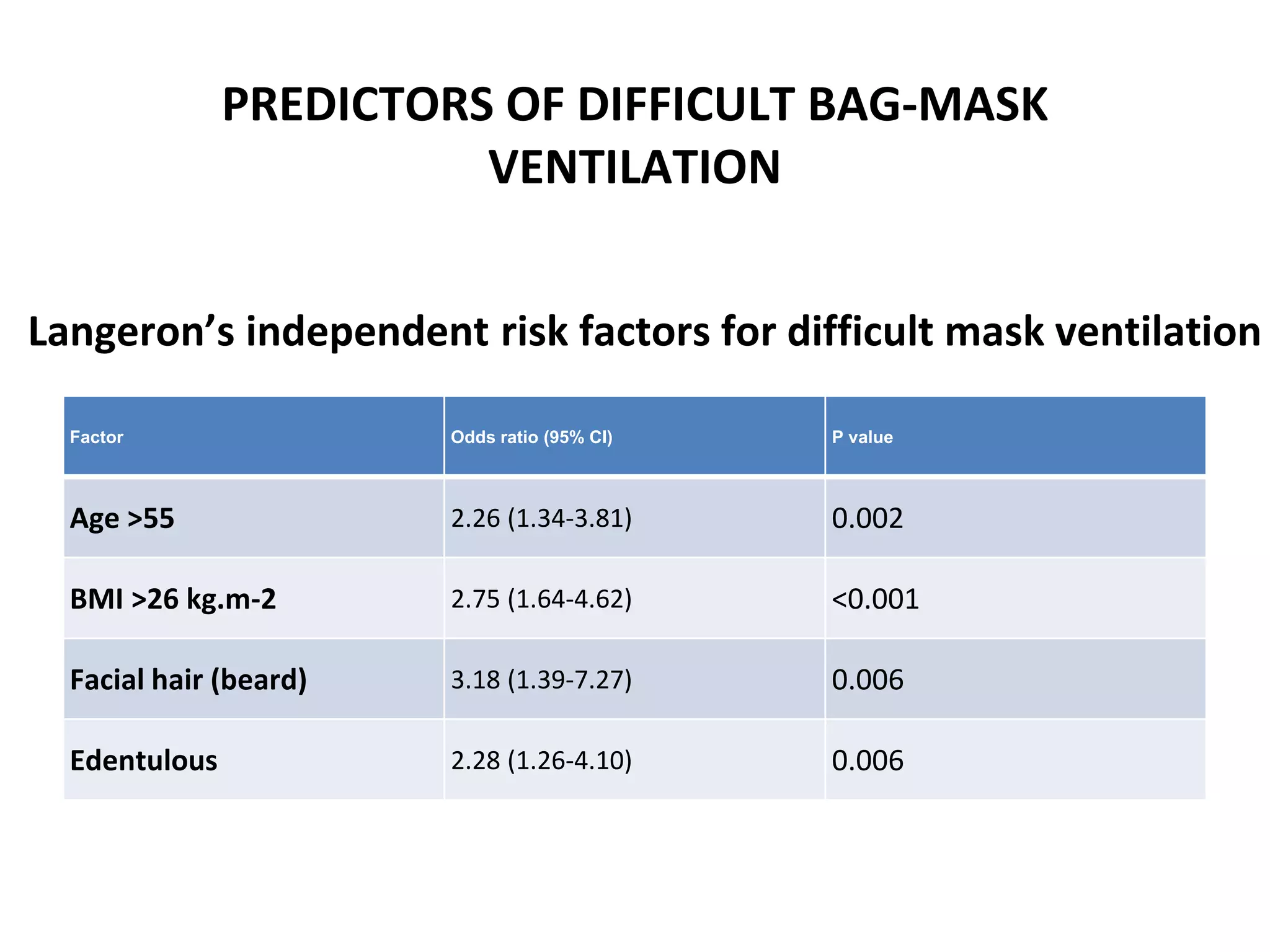
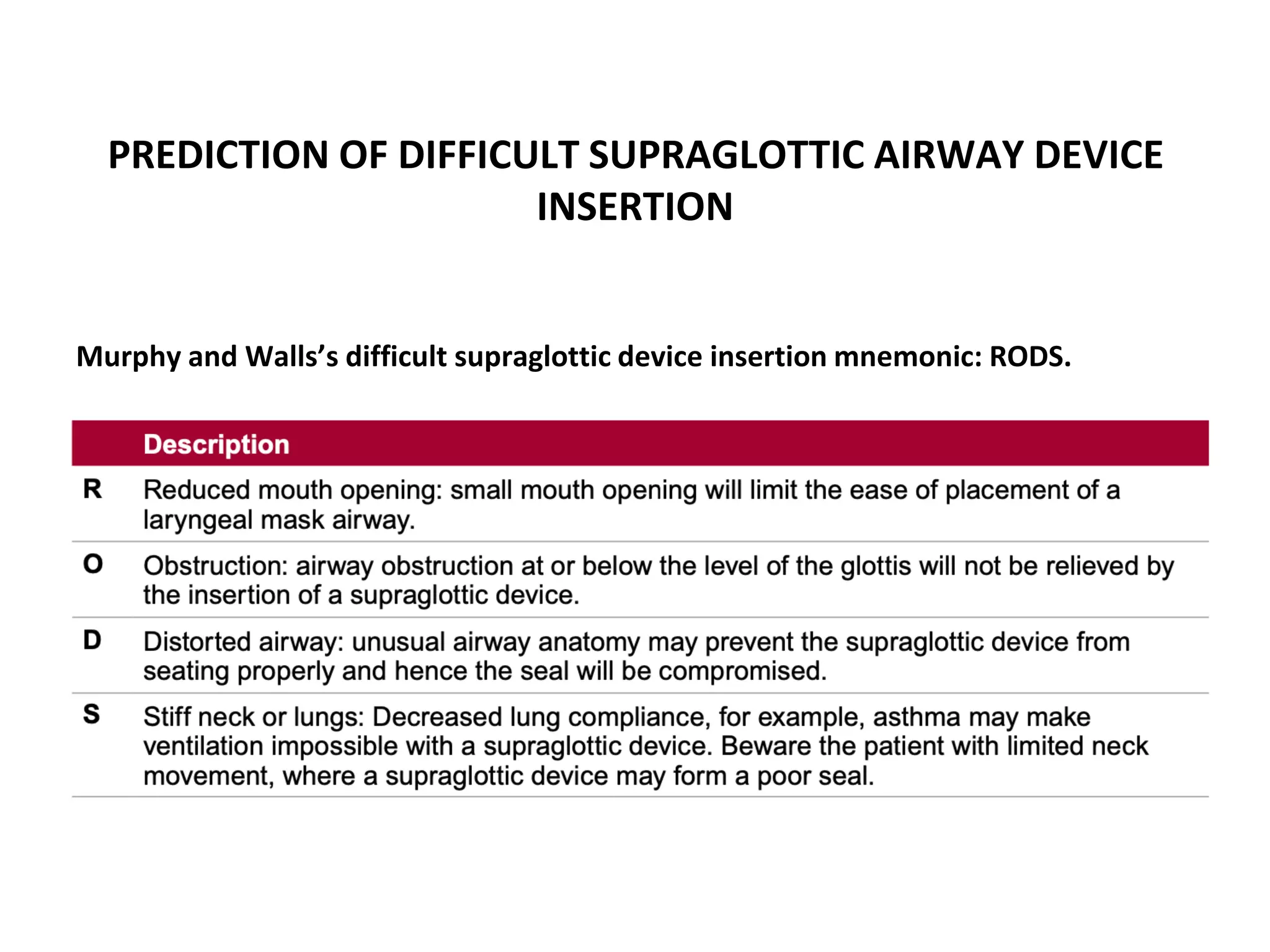
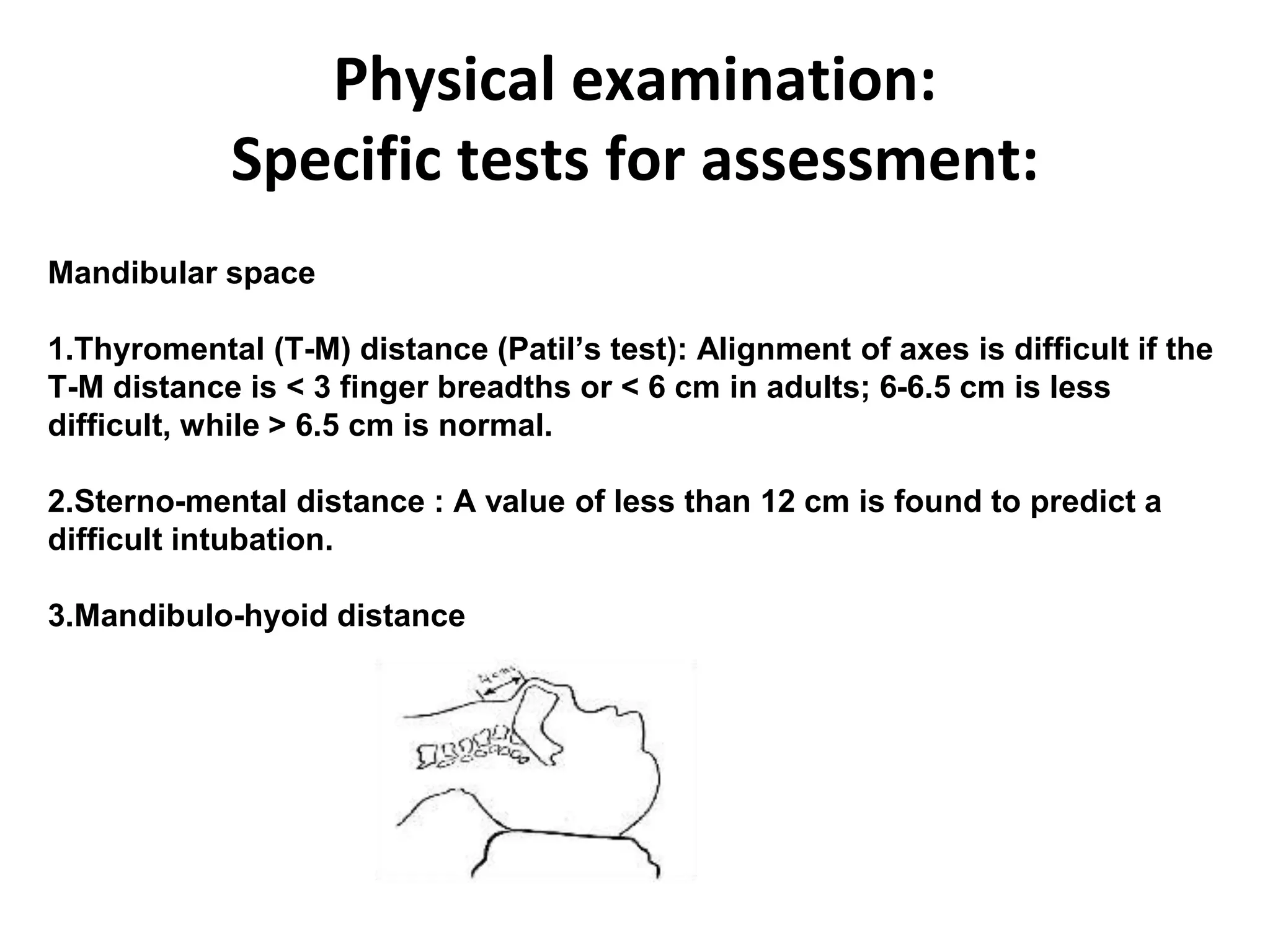
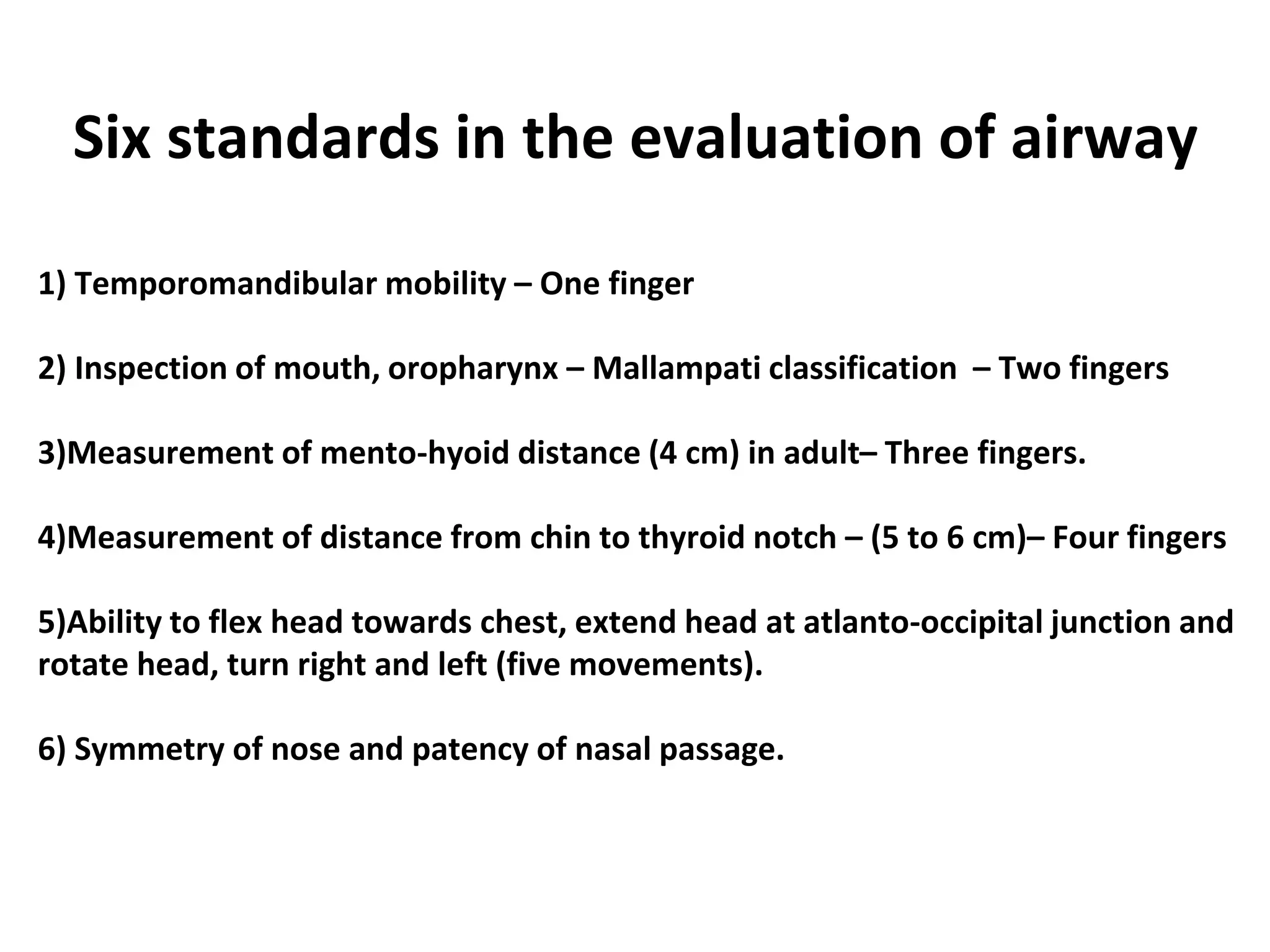
This document provides information on predicting and evaluating difficult airways. It defines different types of difficult airways including difficult bag mask ventilation, difficult supraglottic airway device insertion, and difficult endotracheal intubation. Risk factors for difficult bag mask ventilation include age over 55, BMI over 26, facial hair, being edentulous, and a small thyromental distance. The Mallampati score and measurements of mandibular space can help predict difficult direct laryngoscopy. A full airway examination involves assessing the patient's history, mouth opening, neck mobility, jaw movement, and nasal patency.