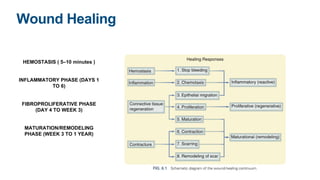
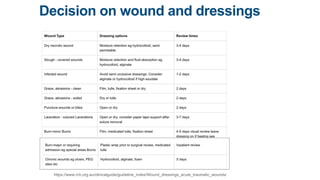
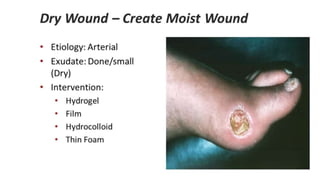
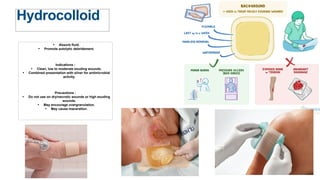
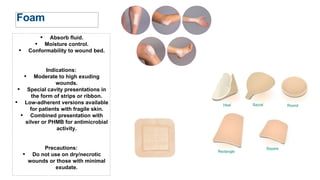
This document discusses wound dressings and their uses. It begins by outlining the four phases of wound healing: hemostasis, inflammatory, proliferative, and maturation. It then discusses the benefits of moisture and warmth in wound healing. Various types of dressings are described, including hydrocolloid, hydrogel, foam, alginates, films, and medicated dressings containing silver or iodine. Factors such as exudate level and wound characteristics are outlined in selecting the appropriate dressing type. The document concludes by mentioning wound drainage needs, pressure sores, and references used.