Downloaded 34 times
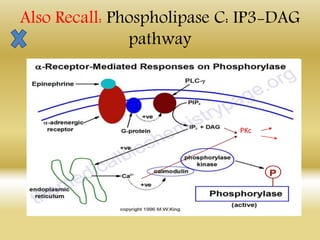
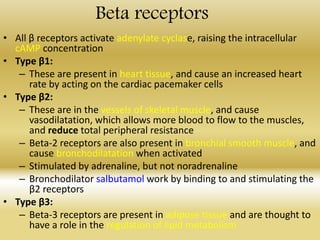
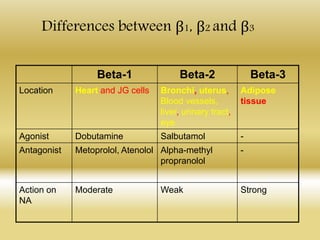
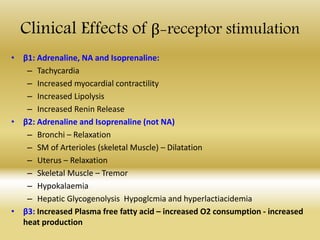
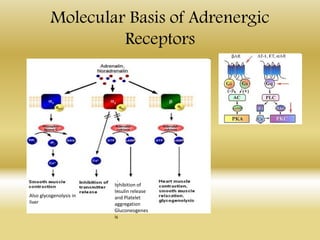
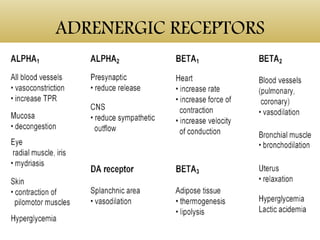
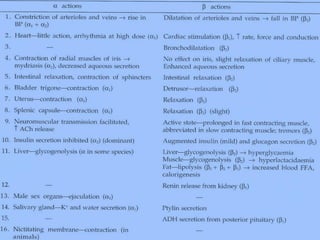

(1) Adrenergic receptors are G-protein coupled receptors that bind catecholamines like adrenaline and noradrenaline. (2) There are two main types - alpha and beta receptors, which are further divided into subtypes. (3) Alpha receptors activate phospholipase C, raising IP3 and DAG, while beta receptors activate adenylate cyclase, raising cAMP. (4) The receptor subtypes are located in different tissues and have different functions, such as vasoconstriction, bronchodilation, increased heart rate, and lipid metabolism.





























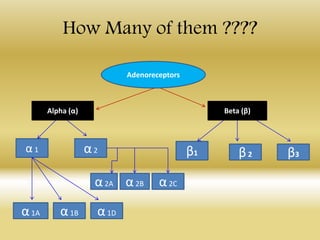
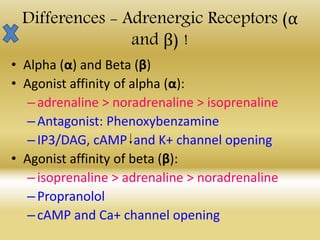
![Adrenergic_Receptors_Enhanced_15_Slides[2].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/adrenergicreceptorsenhanced15slides2-260121162837-2ca10145-thumbnail.jpg?width=640&height=640&fit=bounds)
























































