Downloaded 169 times

![www.wrightington.com
What is a significant
Hill-sachs lesion?
Bigliani & Flatow (1996)
[quoted in Cetik (2007)]:
Mild - <20%
Moderate - 20-45%
Severe - >45%
11
> 30% = Needs Treatment](https://image.slidesharecdn.com/addressingbonelossininstability-lennardfunk-150118044212-conversion-gate01/85/Addressing-bone-loss-in-shoulder-instability-lennard-funk-11-320.jpg)

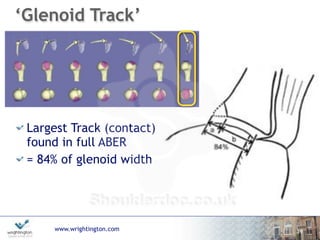
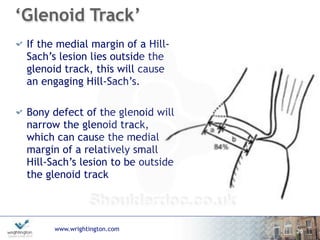
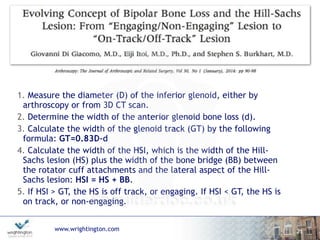
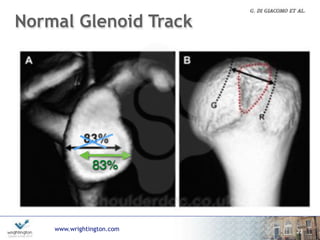
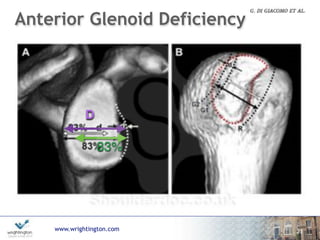
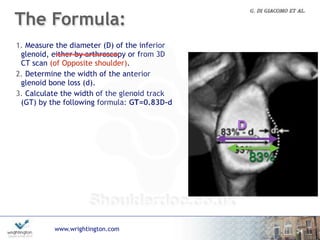

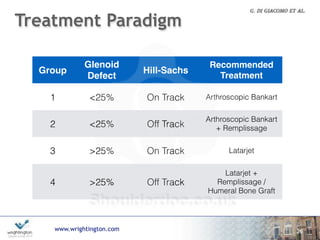




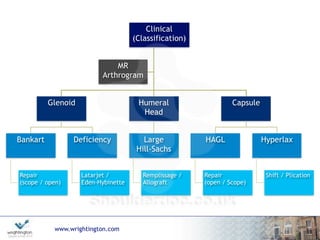


This document discusses approaches to measuring and treating bone loss in the glenoid and humeral head that can contribute to shoulder instability. It addresses how to measure glenoid and Hill-Sachs lesions using various imaging modalities and arthroscopy. It presents studies examining the amount of glenoid and humeral head bone loss that significantly increases instability risk. The document also introduces the "glenoid track" and "Funky Pizza method" to assess if a Hill-Sachs lesion is engaging or non-engaging. It concludes with an overview of treatment approaches based on the size of glenoid and Hill-Sachs defects.




















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















