Downloaded 10 times



![References
• Buchbinder
R,
Green
S,
Forbes
A,
Hall
S,
Lawler
G.
Arthrographic
joint
distension
with
saline
and
steroid
improves
func.on
and
reduces
pain
in
pa.ents
with
painful
s.ff
shoulder:
results
of
a
randomised
double-‐
blind
placebo-‐controlled
trial.
Annals
of
Rheuma*c
Disease
2004;63:302-‐9.
• Corbeil
V,
Dussault
R,
Leduc
B,
Fleury
J.
Adhesive
capsuli.s
of
the
shoulder:
a
compara.ve
study
of
arthrography
with
intra-‐ar.cular
cor.cotherapy
and
with
or
without
capsular
distension
[Capsulite
retrac.le
de
l'epaule:
etude
compari.ve
de
l'arthrographie
avec
cor.cotherapie
intra-‐ar.culaire
avec
ou
sans
distension
capsulaire].
Canadian
Associa*on
of
Radiologists
Journal
1992;43:127-‐30.
• Gam
AN,
Schydlowsky
P,
Rossel
I,
Remvig
L,
Jensen
EM.
Treatment
of
"frozen
shoulder"
with
distension
and
glucocor.coid
compared
with
glucocor.coid
alone.
Scandinavian
Journal
of
Rheumatology
1998;27:425-‐30.
• Jacobs
L,
Barton
M,
Wallace
W,
Ferrousis
J,
Dunn
W,
Bossingham
D.
Intra-‐ar.cular
distension
and
steroids
in
the
management
of
capsuli.s
of
the
shoulder.
BMJ
1991;302:1498-‐501.
• Khan
AA,
Mowla
A,
Shakoor
MA,
Rahman
MR.
Arthrographic
distension
of
the
shoulder
joint
in
the
management
of
frozen
shoulder.
Mymensingh
Medical
Journal
2005;14:67-‐70.
• Andren
L,
Lunderber
B.
Treatment
of
rigid
shoulders
by
joint
distension
during
arthrography.
Acta
Orthopaedica
Scandanavia
1965;36:45-‐53.
• Hsu
S,
Chan
K.
Arthroscopic
distension
in
the
management
of
frozen
shoulder.
Interna*onal
Orthopaedics
1991;15:79-‐83.
• Rizk
TE,
Gavant
ML,
Pinals
RS.
Treatment
of
adhesive
capsuli.s
(frozen
shoulder)
with
arthrographic
capsular
distension
and
rupture.
Archives
of
Physical
Medicine
and
Rehabilita*on
1994;75:803-‐7.
• Anton
HA.
Frozen
shoulder.
Canadian
Family
Physician
1993;39:1773-‐7.
• Arroll
B,
Goodyear-‐Smith
F.
Cor.costeroid
injec.ons
for
painful
shoulder:
a
meta-‐analysis.
Bri*sh
Journal
of
General
Prac*ce
2005;55:224-‐8.
• Binder
AI,
Bulgen
DY,
Hazleman
BL,
Roberts
S.
Frozen
shoulder:
a
long-‐term
prospec.ve
study.
Annals
of
Rheuma*c
Disease
1984;43:361-‐4.
• Buchbinder
R,
Green
S,
Youd
JM.
Cor.costeroid
injec.ons
for
shoulder
pain.
Cochrane
Database
of
Systema*c
Reviews
2003,
Issue
2.
[Art.
No.:
CD004016.
DOI:
10.1002/14651858.CD004016]
• Buchbinder
R,
Youd
J,
Green
S,
Stein
A,
Forbes
A,
Harris
Bennell
K,
et
al.
Efficacy
and
cost-‐effec.veness
of
physiotherapy
following
glenohumeral
joint
distension
for
adhesive
capsuli.s:
A
randomized
trial.
Arthri*s
Care
Research
2007;57(6):1027-‐37.
• Care|e
S,
Moffet
H,
Tardiff
J,
Besse|e
L,
Morin
F,
Fremont
P,
et
al.
Intraar.cular
cor.costeroids,
supervised
physiotherapy,
or
a
combina.on
of
the
two
in
the
treatment
of
adhesive
capsuli.s
of
the
shoulder.
Arthri*s
and
Rheuma*sm
2003;48:829-‐38.
• Cates
C.
Visual
Rx.
h|p://www.nntonline.net/
(accessed
27
June
2007).
• Codman
EA.
The
Shoulder.
Boston:
Thomas
Toddog,
1934.
• Duplay
S.
De
la
peri-‐arthrite
scapulo-‐humerale
et
ces
raideurs
de
l'epaule
qui
en
sont
la
consequence
[De
la
peri-‐arthrite
scapulo-‐humerale
et
ces
raideurs
de
l'epaule
qui
en
sont
la
consequence].
Archives
General
Medicine
1872;20:513.
• Ekelund
A,
Rydell
N.
Combina.on
treatment
for
adhesive
capsuli.s
of
the
shoulder.
Clinical
Orthopaedics
and
Related
Research
1992;282:105-‐9.
• Fareed
DO,
Gallivan
WR,
Jr.
Office
management
of
frozen
shoulder
syndrome:
treatment
with
hydraulic
distension
under
local
anesthesia.
Clinical
Orthopaedics
and
Related
Research
1989;242:177-‐83.
• Gavant
ML,
Rizk
TE,
Gold
RE,
Flick
PA.
Disten.on
arthrography
in
the
treatment
of
adhesive
capsuli.s
of
the
shoulder.
Journal
of
Vascular
Interven*onal
Radiology
1994;5(2):305-‐8.
• Green
S,
Buchbinder
R,
Forbes
A,
Glazier
R.
Systema.c
review
of
randomised
controlled
trials
of
interven.ons
for
painful
shoulder:
selec.on
criteria,
outcome
assessment,
and
efficacy.
BMJ
1998;16:354-‐60.
• Green
SE,
Buchbinder
R,
Forbes
A,
Glazier
R.
Interven.ons
for
shoulder
pain.
Cochrane
Database
of
Systema*c
Reviews
1999,
Issue
2.
[Art.
No.:
CD001156.
DOI:
10.1002/14651858.CD001156]
• Hazleman
BL.
The
painful
s.ff
shoulder.
Rheumatology
and
Physical
Medicine
1972;11(8):413-‐21.
• Higgins
JPT,
Green
S,
editors.
Loca.ng
and
selec.ng
studies.
Cochrane
Handbook
for
Systema.c
Reviews
of
Interven.ons
4.2.5
[updated
May
2005];
Sec.on
5.
www.cochrane.org/resources/handbook/hbook.htm
(accessed
24
November
2006).
• Lundberg
B.
The
frozen
shoulder.
Acta
Orthopaedica
Scandanavia
1969;119:5-‐59.
• Moher
D,
Schulz
K,
Altman
DG
for
the
CONSORT
Group.
The
CONSORT
statement:
revised
recommenda.ons
for
improving
the
quality
of
reports
of
parallel
group
randomized
trials
2001.
h|p://www.consort-‐
statement.org/Statement/revisedstatement.htm
(accessed
27
June
2007).
• Neviaser
JS.
Adhesive
capsuli.s
of
the
shoulder:
a
study
of
the
pathological
findings
in
periarthri.s
of
the
shoulder.
Journal
of
Bone
and
Joint
Surgery
1945;27:211-‐22.
– Web
of
Science®
Times
Cited:
157
• Neviaser
TJ.
Adhesive
capsuli.s.
Orthopedic
Clinics
of
North
America
1987;18:439-‐43.
• Reeves
B.
The
natural
history
of
the
frozen
shoulder
syndrome.
Scandinavian
Journal
of
Rheumatology
1975;4:193-‐6.
• Simmonds
F.
Shoulder
pain
with
par.cular
reference
to
'frozen'
shoulder.
Journal
of
Bone
and
Joint
Surgery
1949;318:426-‐32.
• Tugwell
P,
Shea
B,
Boers
M,
Simons
L,
Strand
V,
Wells
G.
Evidence-‐based
Rheumatology.
BMJ
Books,
2003.
• van
der
Windt
DA,
Koes
BW,
de
Jong
BA,
Bouter
LM.
Shoulder](https://image.slidesharecdn.com/hydrodistensiondebate-abasrashid-150118044416-conversion-gate01/85/Hydrodistension-debate-abas-rashid-12-320.jpg)

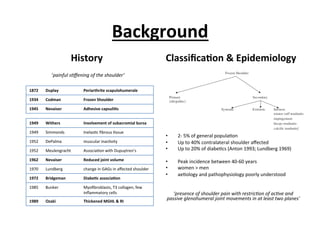
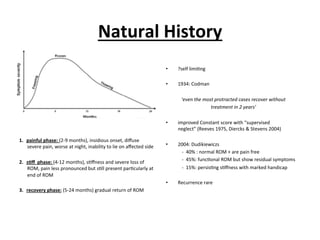
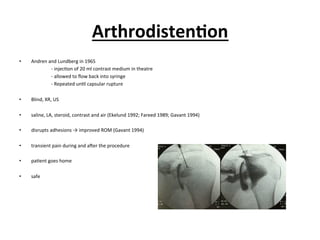
This document summarizes the debate around adhesive capsulitis and hydrodistension treatment. It provides background on the classification, epidemiology, and natural history of adhesive capsulitis. It then discusses the development of arthrodistension/hydrodistension treatment, including early studies from the 1960s. The 2006 Cochrane Review on this topic is summarized, which identified 4 randomized controlled trials comparing arthrodistension to other treatments. The review found arthrodistension provided short-term improvements in pain and range of motion compared to placebo or other interventions.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
