Download as PDF, PPTX
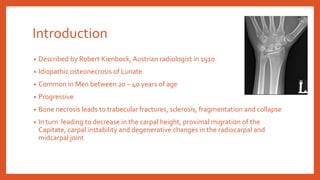







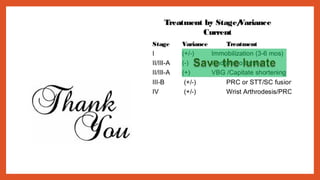


Mr. Kiran Kumar Naikoti's document describes Kienbock's disease, an idiopathic osteonecrosis of the lunate bone that commonly affects men aged 20-40. The disease is progressive and results from bone necrosis leading to fractures, sclerosis, and collapse of the lunate bone. This in turn causes decreased carpal height, proximal capitate migration, carpal instability, and degenerative wrist changes. The etiology is multifactorial and may involve trauma, anatomical factors like negative ulnar variance, vascular causes like single vessel lunate supply, and systemic diseases. Stages of the disease are described based on radiological findings from normal to severe lunate collapse. Treatment options discussed include














































































