Downloaded 383 times











![Ethics
“THE UNWRITTEN RULES OF LIFE THAT KEEP BALANCE “
LIVE BY THE RULES....
eth⋅ics
[eth-iks]
• –plural noun
• 1.(used with a singular or plural verb ) a system of moral
principles: the ethics of a culture.
• 2.the rules of conduct recognized in respect to a
particular class of human actions or a particular group,
culture, etc.: medical ethics; Christian ethics.
• 3.moral principles, as of an individual: His ethics forbade
betrayal of a confidence.
• 4.(usually used with a singular verb ) that branch of
philosophy dealing with values relating to human
conduct, with respect to the rightness and wrongness of
certain actions and to the goodness and badness of the
motives and ends of such actions.
ETHICS ARE AN INTEGRAL AND IMPERATIVE
COMPONENT IN NURSING
ETHICS ARE NON NEGOTIABLE](https://image.slidesharecdn.com/orientationredone-121011210424-phpapp01/85/Orientation-to-Home-Care-Nursing-16-320.jpg)


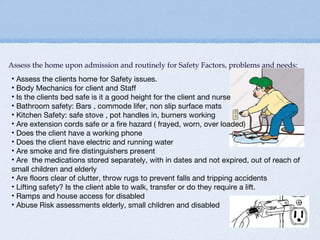
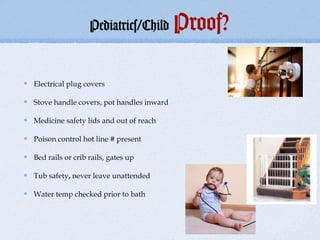






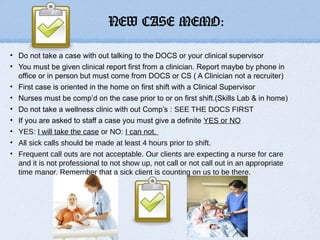








This orientation document provides an overview of key differences between home care and facility care environments. It also summarizes the roles and responsibilities of home care nurses, including administering medications, documenting in patient charts and on flow sheets, reconciling medications, and following physician orders as outlined in the plan of care (485 form). Proper documentation, medication administration, and communication with physicians are emphasized.













































































