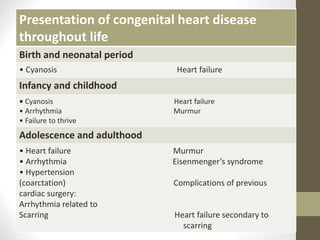
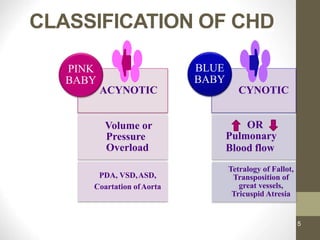
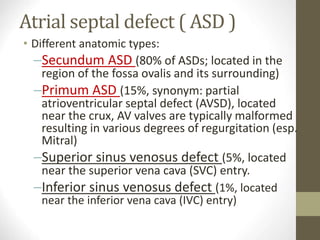
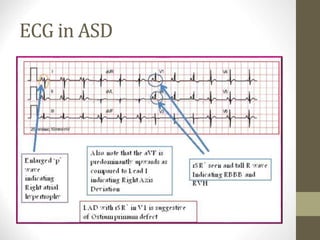
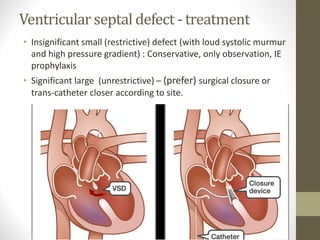
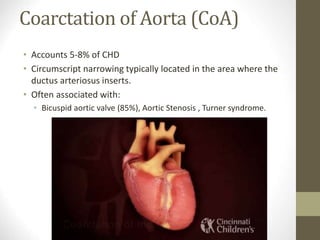
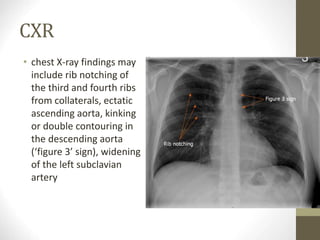
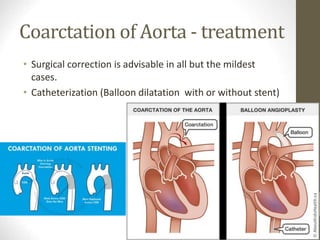
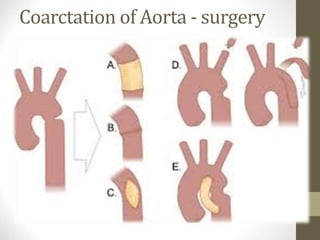
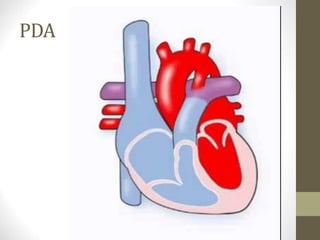
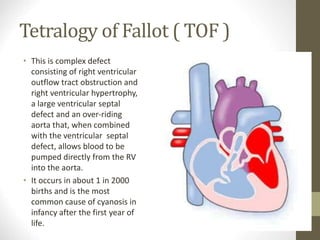
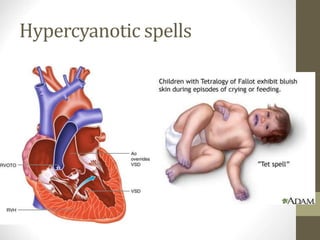
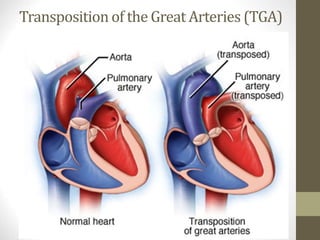
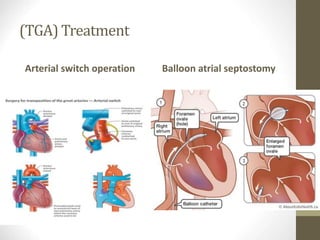
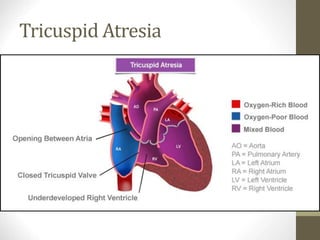
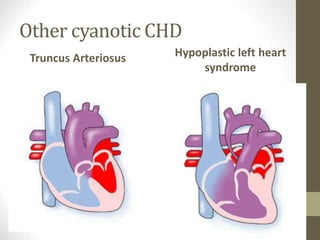
This document provides information on congenital heart disease (CHD), including epidemiology, classification, diagnosis, and treatment. It discusses several specific types of CHD such as atrial septal defect (ASD), ventricular septal defect (VSD), patent ductus arteriosus (PDA), coarctation of the aorta, tetralogy of Fallot, transposition of the great arteries, tricuspid atresia, truncus arteriosus, and hypoplastic left heart syndrome. It describes the clinical presentation, investigations, and management approaches for each condition.