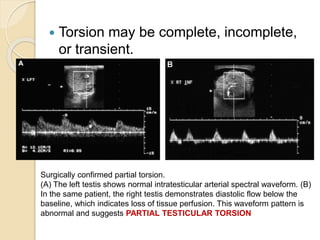
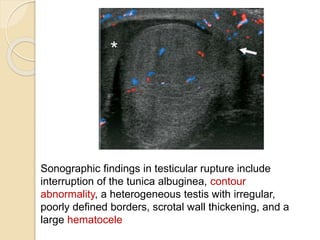
This document summarizes the use of ultrasound in evaluating acute scrotal pain. It describes the normal anatomy and vascular supply of the scrotum and then discusses various pathologies that can cause acute scrotal pain like epididymo-orchitis, testicular torsion, varicocele, trauma and tumors. Epididymo-orchitis is the most common cause of acute scrotum. Ultrasound is useful for diagnosing the specific condition causing pain by identifying features like enlarged epididymis, lack of blood flow in a twisted testis, or intratesticular fluid in an abscess. Color Doppler ultrasound in particular helps evaluate blood flow and make an accurate diagnosis to guide appropriate treatment.

























































![imaging of scrotum [Repaired] [Repaired].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/imagingofscrotumrepairedrepaired-230522050410-51cee1e6-thumbnail.jpg?width=640&height=640&fit=bounds)





























