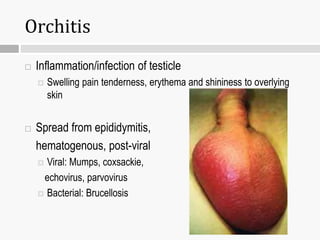
Liam felt a sharp pain in his right testicle after a football game. In the locker room, his right testis was higher than the left and extremely tender. His coach noticed Liam walking slowly with a protective gait and sent him to the hospital for possible emergency surgery. Liam is exhibiting signs and symptoms of testicular torsion including sudden severe scrotal pain, elevated and tender testis, nausea, and inability to walk normally. Testicular torsion requires urgent surgical intervention to detorse the testis within 6-24 hours to save viability. The coach recognized the potential medical emergency and ensured Liam received prompt evaluation and treatment.






















![Abdominal percussion [2015]](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalpercussion2015-151117012348-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)























































