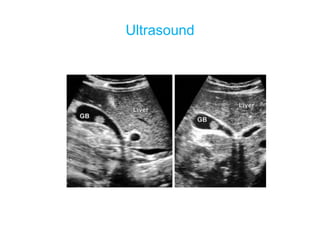
This document discusses acute cholecystitis, which is inflammation of the gallbladder commonly caused by an impacted gallstone obstructing the cystic duct. It presents the typical causative bacteria, clinical features including pain and fever, investigations such as ultrasound and CT scan, complications, differential diagnoses, and treatments including antibiotics and cholecystectomy. It also briefly covers empyema gallbladder, which is acute cholecystitis with pus in the gallbladder, and mucocele of the gallbladder, which is gallbladder distention without infection due to cystic duct obstruction.