- Acute appendicitis is caused by obstruction of the appendix lumen, which leads to mucosal ischemia and bacterial overgrowth. Common symptoms include abdominal pain localized to the right lower quadrant.
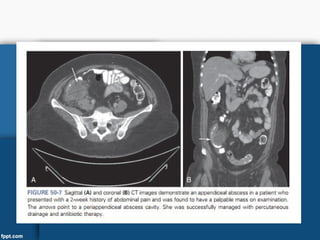
- Diagnosis is typically made through physical exam finding tenderness over McBurney's point and laboratory tests showing leukocytosis. CT scan is the most accurate imaging study, showing a thickened appendix over 7mm in diameter.
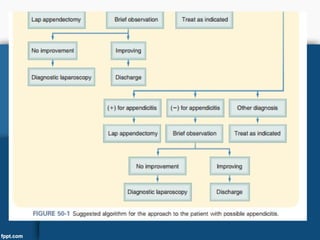
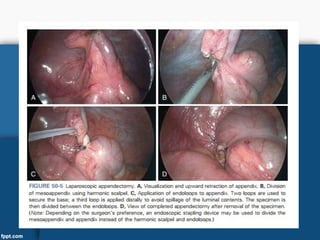
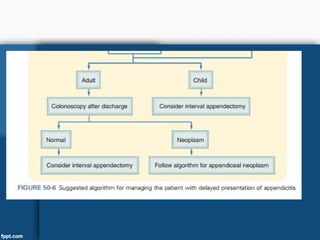
- Treatment involves prompt surgical removal of the appendix (appendectomy) which can be performed open or laparoscopically. Antibiotics are given before and after surgery. For perforated appendicitis, broader antibiotic coverage is needed and surgery remains the standard