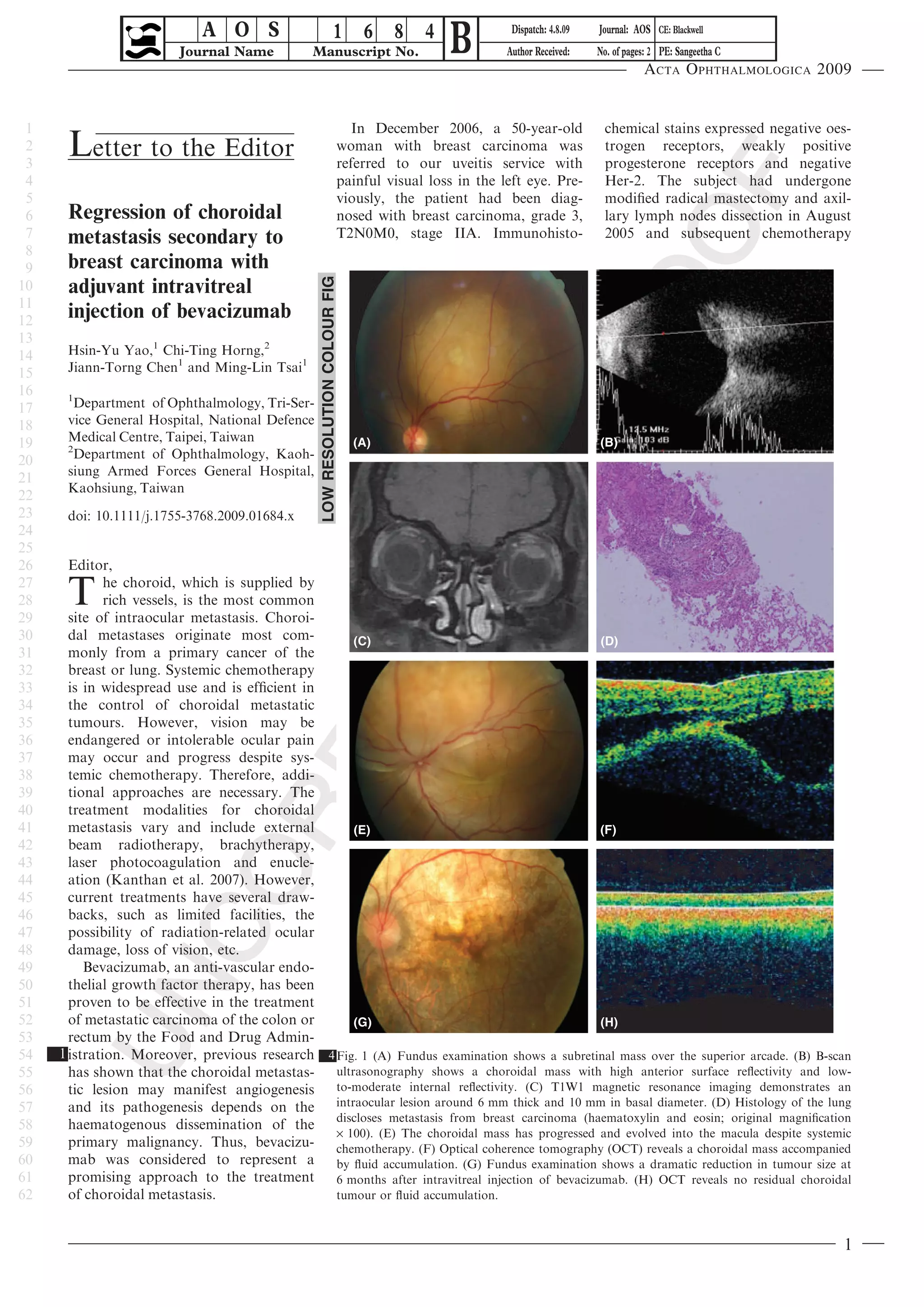
This letter discusses a case study of a 50-year-old woman with breast cancer who developed a choroidal metastasis in her left eye. Systemic chemotherapy was ineffective at controlling the growth of the choroidal lesion. She received an intravitreal injection of bevacizumab, which led to significant regression of the choroidal tumor over a 6 month period with no recurrence over 24 months of follow up. The letter suggests intravitreal bevacizumab may be an effective treatment for choroidal metastases when systemic chemotherapy proves insufficient.


















![[3]Radionuclides_Surgery](https://cdn.slidesharecdn.com/ss_thumbnails/1664463-thumbnail.jpg?width=640&height=640&fit=bounds)











![2009 Convegno Malattie Rare Buzio [23 01]](https://cdn.slidesharecdn.com/ss_thumbnails/2009convegnomalattierarebuzio2301-090330153412-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)

























![Avastine150.full[1]](https://cdn.slidesharecdn.com/ss_thumbnails/avastine150-140715032805-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)













![20120510(print台科大) 醫學工程於鑑識科學的應用60min [相容模式]](https://cdn.slidesharecdn.com/ss_thumbnails/20120510print60min-120504032951-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)































