Acute Coronary Syndrome
•Download as PPTX, PDF•
40 likes•2,805 views

The document discusses acute coronary syndrome (ACS), which includes unstable angina, non-ST-segment elevation myocardial infarction (NSTEMI), and ST-segment elevation myocardial infarction (STEMI). It focuses on angina pectoris, describing the three main types as stable angina, unstable angina, and Prinzmetal angina. Risk factors for angina are discussed, including modifiable factors like hypertension, smoking, and high cholesterol. The pathophysiology of angina and differences between NSTEMI, STEMI, and unstable angina are summarized.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Acute Coronary Syndrome
Similar to Acute Coronary Syndrome (20)
Recently uploaded
Recently uploaded (20)
Acute Coronary Syndrome
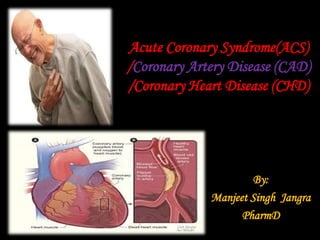
- 1. Acute Coronary Syndrome(ACS) /Coronary Artery Disease (CAD) /Coronary Heart Disease (CHD) By: Manjeet Singh Jangra PharmD
- 2. • Acute coronary syndrome (ACS) is the umbrella term for the clinical signs and symptoms of myocardial Ischemia: unstable angina, non–ST- segment elevation myocardial infarction (Non- STEMI), and ST-segment elevation myocardial infarction (STEMI). • Here we will discuss the following chapters in details: Angina Pectoris Myocardial Infarction
- 4. Introduction • Angina pectoris is a clinical syndrome that occurs when low blood flow to the heart (myocardial ischemia) limits delivery of oxygen to the heart muscle during exertion. • It is felt as discomfort and tightening in the chest that is sometimes accompanied by pain in the left arm, shoulders, or jaw. • Usually, blood flow is decreased because of blockage within one or more of the coronary arteries supplying the heart muscle (coronary artery disease). • Its risk increase with age , smoking, hypertension, hypercholesterolemia, diabetes.
- 5. Types of Angina The various forms are divided into three basic types: 1. Stable angina: in which pain is present only during exertion or extreme emotional distress and disappears with rest; 2. Unstable angina: in which symptoms occur with increasing frequency and pain occurs more easily at rest, feels more severe, or lasts longer; and 3. Prinzmetal angina, in which angina occurs at rest, when sleeping, or when exposed to cold temperatures. In the latter type of angina, symptoms are generally caused by transient spasms of the coronary artery rather than by actual blockage of the artery by plaque or clots.
- 7. Risk Factors Non-modifiable Risk factors include age, sex, family history, and ethnicity or race. Men have a higher risk than women. Men older than age 45, women older than age 55, and anyone with a first-degree male or female relative who developed coronary artery disease before age 55 or 65, respectively, are also at increased risk. Modifiable risk factors include elevated levels of serum cholesterol, low-density lipoprotein cholesterol, and triglycerides; lower levels of high-density lipoprotein cholesterol; and the presence of type 2 diabetes, cigarette smoking, obesity, a sedentary lifestyle, hypertension, and stress
- 9. Pathophysiology • Usually, blood flow is decreased because of blockage within one or more of the coronary arteries supplying the heart muscle (coronary artery disease). • This blockage is typically the result of a buildup of fatty deposits (plaque) that gradually block the flow of blood and oxygen in the artery (atherosclerosis).
- 10. • Atherosclerotic narrowing of the coronary artery is the most frequent source of cardiac ischemia and angina; however, endothelial damage or dysfunction in the heart, a sudden tightening or narrowing of the coronary artery (vasospasm), or severe narrowing of the aortic valve (aortic stenosis) may also interfere with coronary blood flow, reduce delivery of oxygen to heart tissue, and cause angina. • Angina can also be caused by other mechanisms that reduce oxygen delivery, such as anemia (low red blood cell count and/or low hemoglobin), low blood pressure (hypotension), bradycardia, exposure to carbon monoxide, and inflammation.
- 15. Unstable Angina Cause • Thrombus partially or intermittently occludes the coronary artery Signs and Symptoms • Pain with or without radiation to arm, neck, back, or epigastric region • SOB, diaphoresis, nausea, lightheadedness, tachycardia, tachypnea, hypotension or hypertension, decreased arterial oxygen saturation (SaO2) rhythm abnormalities ; Occurs at rest or with exertion; limits activity Diagnostic Findings: ST-segment depression or T-wave inversion on electrocardiography (ECG); Cardiac biomarkers not elevated. Treatment (MONA-BAH) • Oxygen to maintain oxygen saturation level at > 90% • Nitroglycerin or morphine to control pain • b-blockers, ACE inhibitors, statins (started on admission and continued long term), clopidogrel, unfractionated heparin or LMWH, and glycoprotein IIb/IIIa inhibitors
- 16. Non–ST-Segment Elevation Myocardial Infarction (NSTEMI) Cause: Thrombus partially or intermittently occludes the coronary artery Signs and Symptoms: Pain with or without radiation to arm, neck, back, or epigastric region, SOB, diaphoresis, nausea, lightheadedness, tachycardia, tachypnea, hypotension or HTN, ↓ed arterial oxygen saturation (SaO2) and rhythm abnormalities. • Occurs at rest or with exertion; limits activity; Longer in duration and more severe than in unstable angina Diagnostic Findings: ST-segment depression or T-wave inversion on electrocardiography; Cardiac biomarkers are elevated Treatment (MONA-BAH, PCI): • Oxygen to maintain SaO2 level at > 90% • Nitroglycerin or morphine to control pain • b-blockers, ACEI, statins (started on admission and continued long term), clopidogrel, unfractionated heparin or LMWH, and glycoprotein IIb/IIIa inhibitors • Cardiac catheterization and possible PCI for patients with ongoing chest pain, hemodynamic instability, or increased risk of worsening clinical condition
- 17. ST-Segment Elevation Myocardial Infarction (STEMI) Cause: Thrombus fully occludes the coronary artery Signs and Symptoms: Pain with or without radiation to arm, neck, back, or epigastric region, SOB, diaphoresis, nausea, lightheadedness, tachycardia, tachypnea, hypotension or hypertension, decreased arterial O2 saturation (SaO2), and rhythm abnormalities; Occurs at rest or with exertion; limits activity, Longer in duration and more severe than in unstable angina (irreversible tissue damage [infarction] occurs if perfusion is not restored) Diagnostic Findings: ST-segment elevation or new left bundle branch block on ECG. Cardiac biomarkers are elevated Treatment: (TPA, MONA-BAH, PCI): Fibrinolytic therapy within 30 minutes of medical evaluation, Oxygen to maintain SaO2 level at > 90% • Nitroglycerin or Morphine to control pain • BB, ACEI, statins (started on admission & continued long term), clopidogrel, unfractionated heparin or LMWH • PCI within 90 minutes of medical evaluation
- 18. Some common ECG changes in AMI