Introduction
• Abortion isone of the leading
cause of maternal mortality it
accounts
• 13% world wide
• 4% in Africa
3.
Definition
Abortion isexpulsion of the products
of conception prior to viability of the
fetus (before 28 weeks of gestation) or
less than 1000gm weight
WHO gest. age<20 weeks or weight
less than 500 gm.
4.
ABORTIONS CAN BEclassified as:
• Spontaneous or induced
• First trimester or second trimester
Induced abortion can be legal or
criminal.
Most criminal abortions are unsafe.
5.
Types of abortion
•Spontaneous
• Induced
Spontaneous abortion defined as the
loss of a fetus during pregnancy due to
natural causes…before fetal
development has reached 28 weeks…the
term spontaneous abortion refers to
naturally occurring events, not elective
or therapeutic abortion procedures…”
6.
Types of abortion…..
•Unsafe abortion :-is characterized by lack or
inadequate of skill of provider, hazardous
technique and unsanitary facilities or both
• Therapeutic abortion :-termination of
pregnancy before the time of fetal viability for
the purpose of saving the life of the mother
7.
Etiology of spontaneousabortions
Could be classified into fetal and maternal
factors
A) Fetal anomaly
– Chromosomal
– Structural
– Genetic
B) Maternal disease
- pyrexia
- Diabetes mellitus
- Thyroid disease
8.
Etiology …
C) Endocrinedisorder
- early luteal phase defect
D) Uterine abnormalities
- fibroids, especially sub mucous
- congenital uterine anomalies
- intrauterine adhesions
- low implantation of the placenta
Cont..
• Septic abortion:-whenany of the stage of
abortion complicated by pelvic infection
• Recurrent abortion:-three or more
consecutive spontaneous termination of
pregnancies
13.
Clinical stages ofabortion
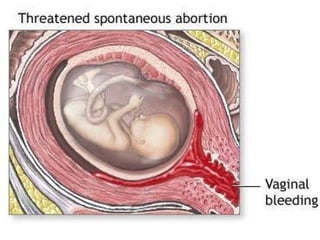
Threatened abortion
oslight intermittent bleeding with or without cramping
o The cervix remains closed and no cervical effacement
oAt least 20–30% of pregnant women have some first-
trimester bleeding.
oIn most cases, this is thought to represent an
implantation bleed.
oMore than 50-80% go to term
15.
Inevitable abortion
Thecervix has dilated, but the products
of conception have not been expelled
Abdominal or back pain and mild to
severe vaginal bleeding
cervical effacement, cervical dilatation,
and/or rupture of the membranes is
noted.
It is Irreversible
16.
Incomplete abortion
• Some,but not all, of the products of
conception have been passed; retained
products may be part of the fetus,
placenta, or membranes
• In gestations of less than 10 weeks'
duration, the fetus and placenta are usually
passed together. After 10 weeks, they may
be passed separately, with a portion of the
products retained in the uterine cavity.
17.
Sign and symptoms
•Cramps are usually present
• Profuse persistent bleeding
• HX of passing concepts tissue
• Some times visible or palpable concepts
tissue through the opening cervix
Complications
Anemia, hemorrhage and infection
18.
Missed abortion
Def. apregnancy in which there is a fetal
demise (usually for a number of weeks) but
no uterine activity to expel the products of
conception
Regress sx/s of pregnancy , Uterine size
decreased, cervix closed, Brownish vaginal
discharge
Complications
Infection, DIC, AF embolism
19.
Complete abortion
• Allproducts of conception have been passed
without need for surgical or medical
intervention.
• Slight bleeding may continue for a short time
• pain usually ceases after pregnancy has
traversed the cervix.
20.
Differential diagnosis
• Idiopathicbleeding in a viable pregnancy
• Ectopic pregnancy
• Molar pregnancy
• Infection of the vagina or cervix
• Cervical abnormalities
–Malignancy, polyps, trauma
• Vaginal trauma
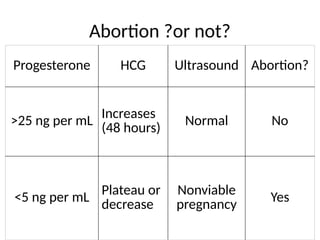
Abortion ?or not?
ProgesteroneHCG Ultrasound Abortion?
>25 ng per mL
Increases
(48 hours)
Normal No
<5 ng per mL
Plateau or
decrease
Nonviable
pregnancy
Yes
23.
Complications
• Severe orpersistent hemorrhage life
threatening.
• Sepsis develops most frequently after self-
induced abortion.
• Intra abdominal injury
- Perforation of the uterine wall may
- injury to the bowel and bladder
• Asherman’s syndrome, also known as intrauterine
adhesions, is a condition where the cavity of the
uterus develops scar tissue (adhesions)
24.
Cont..
. Sheehan syndrome,also known as Simmond syndrome,
postpartum hypopituitarism or postpartum pituitary
gland necrosis, is hypopituitarism (decreased
functioning of the pituitary gland), caused by ischemic
necrosis due to blood loss and hypovolemic
shockduring and after childbirth.
• Multiple pregnancy with the loss of 1 fetus and
retention of another ("vanishing twin").
• Other complications of abortion
Anemia
Renal failure
Infertility(if hysterectomy done
due to complication)
25.
Prevention
• Early obstetriccare
• Treatment maternal disorders like
diabetes and hypertension
• Protection of pregnant women from
environmental hazards and exposure
to infectious diseases.
26.
Laboratory investigations
• Bloodtype and RH factor
• Complete blood count
• HCG to confirm pregnancy
• WBC and differential to rule out
infection
27.
General management
first-trimester loss
MVA,E&D or D&C
After the first trimester
• hospitalization should be considered
• Oxytocics are helpful in contracting the
uterus, limiting blood loss, and aiding in
expulsion of clots and tissue.
Treatment
For treated abortion
Bedrest and pelvic rest
Avoid coitus, douching and strenuous
exercise
• Prognosis is good when bleeding
and/or cramping resolve.
30.
For inevitable abortion
•According to gestational age
<14 weeks MVA
>14weeks oxytocin infusion and
E/C with pethdine or sedative
31.
For incomplete abortion
•Evacuation based on gestational age
• Uterotonic agents
• Blood and fluid replacement
• Antibiotic
• The prognosis for the mother is excellent
if the retained tissue is promptly and
completely evacuated.
32.
For complete abortion
•observed for further bleeding.
• The products of conception should be
examined.
• prognosis for the mother is excellent
33.
For missed abortion
Expectantmanagement
-3-4 weeks follow up
-Clotting profile
>14weeks
-Prostaglandin or balloon catheter to dilate
cervix
-Pitocin
<14 weeks :-MVA or D/c
34.
Treatment of complication
Managedaccordingly
• laparotomy are indicated to determine
the extent of laceration or bowel injury
• Broad spectrum antibiotics for sepsis
35.
Recurrent spontaneous abortion
•Defined as 3 or more consecutive, spontaneous
pregnancy losses before 28 weeks of gestation from
the last menstrual period , by the same partner ,
each with a fetus weighing less than 1000 g.
• Approximately 1% of women are habitual aborters.
• The risk of having a spontaneous abortion for the
first time is about 15%, and this risk is at least
doubled in women experiencing recurrent abortion
36.
Etiology
Three generally acceptedetiologies of
recurrent miscarriages are:-
• Chromosomal abnormalities
• uterine malformations
- bicornuate or septate uterus
- cervical incompetence
• Immunologic Factors
-Antiphospholipid antibodies
37.
Others etiology
• submucous myomas
• Hormonal causes like hyper and
hypothyroidism
• Infection
• Maternal system disease e.g. diabetes
• Chronic malnutrition
38.
Treatments
• Pre implantationdiagnosis, or prenatal
testing on subsequent conceptions.
• Uterine operation: hysteroscopy resection
• Cervical cerclage
• myomectomy.
• Appropriate antibiotics
39.
Induced abortion
Induced abortionis the medical or surgical
termination of pregnancy before the time of fetal
viability. it can be legal or illegal, therapeutic
(safe) or un safe( septic )
septic or Unsafe abortion defined by WHO:
“. . .any procedure for terminating an unwanted
pregnancy (carried out) either by persons
lacking the necessary skills or in an environment
lacking minimal medical standards, or both . . .”
40.
Pathogenesis
• Instrument byillegal abortion or
ascending infection from the vaginal
cavity to normal sterile uterus
41.
Sign and symptoms
•fever, shivering
• malodorous vaginal discharge
• pelvic and abdominal pain
• Rebound tenderness
• cervical motion tenderness.
• Peritonitis and sepsis
42.
Investigations
• A completeblood count
• Hct ,blood group and cross match
• Urine culture and sensitivity
• endometrial cultures
• abdominal x-ray to rule out uterine
perforation should be obtained
• Ultrasound may be helpful in ruling out
retained products of conception.
43.
Management
• Hospitalization andintravenous antibiotic therapy
• Broad spectrum antibiotic (ciprofloxacin+ gentamycin)
• Monitor v/s
• Blood transfusion if Hgb is low
• Remove focus of infection
• T.A.T to prevent tetanus
• Anti D for RH negative
• Post abortion care
• Hysterectomy for pelvic abscess and severe perforation
44.
Post abortion care
PACis an approach for:-
Reducing morbidity and mortality
from complications of unsafe and
spontaneous abortion, and
improving women’s sexual and
reproductive health and lives.
45.
Why is PACan important intervention?
• Saves women’s lives, increases use of FP, and
prevents repeat abortion
• Is acceptable where induced abortion is legally
restricted
• Links curative service (treatment for
complications) with preventive service (FP)
• Should be included in the existing range of
services and should not be a separate , vertical
service
• Can be offered successfully in low resource
settings
46.
Magnitude of theproblem of
unsafe abortion
• About 40-50 million women experience
abortions annually and 50% of these are unsafe
• 13% of maternal mortality–67,000 women–8
women die every hour
• 38 to 68% are less than 20 years old
• 10 to 50% need medical care
• More than 95% of deaths and injuries from
unsafe abortion occur in developing countries.
• ratio of 1 unsafe abortion for every 7 live births
.
47.
Other factors thatcomplicate the problem of
unsafe abortion:-
• Unmet need for contraception to delay, space
or limit pregnancies
• Unmet need for sexually transmitted infection
(STI)/HIV prevention and care
48.
Essential Elements ofPost abortion Care
1. Treatment
• Treat incomplete and un safe abortion and
potentially life threatening complications.
2. Contraceptive and family planning services
• Help women prevent unwanted pregnancy or
practice birth spacing.
49.
cont..
3. Reproductive andother health services
• Preferably provide on - site, or via referrals to
other accessible facilities in provides’ networks.
50.
Cont..
4. Community andservice provider partnerships
• Prevent unwanted pregnancies and unsafe
abortion.
• Mobilize resources to help women receive
appropriate and timely care for complications
from abortion.
1 All ofthe following may be the cause of
recurrent abortion except:
A cervical incompetence
B infection
C chromosome aberrantions
D retroversion of the uterus
54.
2 A patientof 8th week pregnancy, presents
with vaginal bleeding, low abdominal pain,
vaginal examination revealing partially dilatated
cervix, without expelling any tissue, she should
be diagnosed as :
A threatened abortion
B inevitable abortion
C complete abortion
D incomplete abortion





























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







