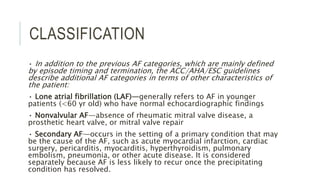
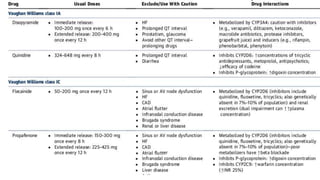
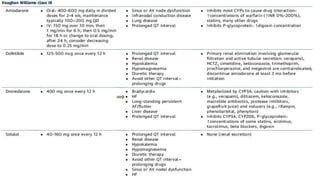
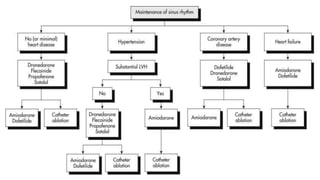
1. The document discusses classification, management, and treatment of atrial fibrillation. It describes classification as paroxysmal, persistent, or permanent based on episode duration.
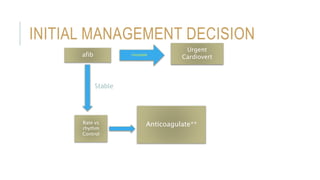
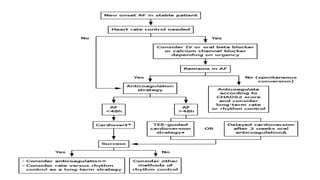
2. For stable patients, the first steps are evaluation, rate control if needed, and decision on cardioversion. For unstable patients, urgent cardioversion may be required. Electrical cardioversion is preferred but drugs can be used.
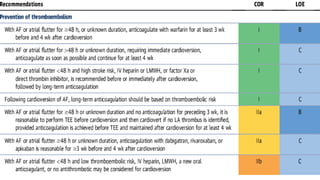
3. Anticoagulation for at least 3 weeks prior to and 4 weeks after cardioversion is recommended for episodes over 48 hours. For episodes under 48 hours, practices vary from anticoagulation in all to risk-based approaches.


![URGENT MANAGEMENT
Three circumstances for which urgent or emergent cardioversion may
be needed include:
●Active ischemia (symptomatic [eg, angina] or electrocardiographic
evidence).
●Evidence of organ hypoperfusion (eg, cold clammy skin, confusion,
acute kidney injury).
●Severe manifestations of heart failure (eg, pulmonary edema)](https://image.slidesharecdn.com/a-fib-150514175706-lva1-app6891/85/A-fib-9-320.jpg)













































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)













