Downloaded 19 times

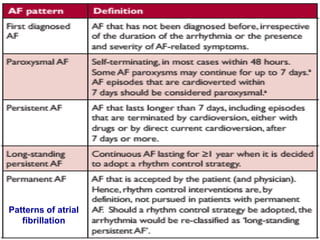
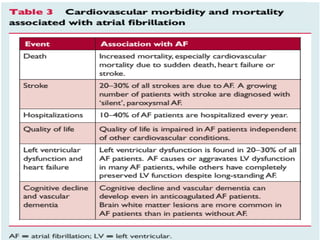


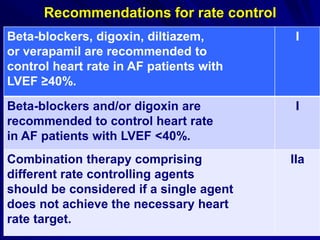
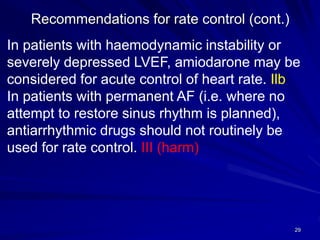

Atrial fibrillation (AF) is a common arrhythmia linked to increased mortality and morbidity. The document discusses the definitions of different types of AF and compares rhythm control versus rate control, finding no significant differences in clinical outcomes, although rhythm control led to more hospitalizations. Recommendations favor rate control as the primary strategy, with rhythm control reserved for specific cases where symptoms persist despite rate management.










































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












