Download as PPSX, PPTX













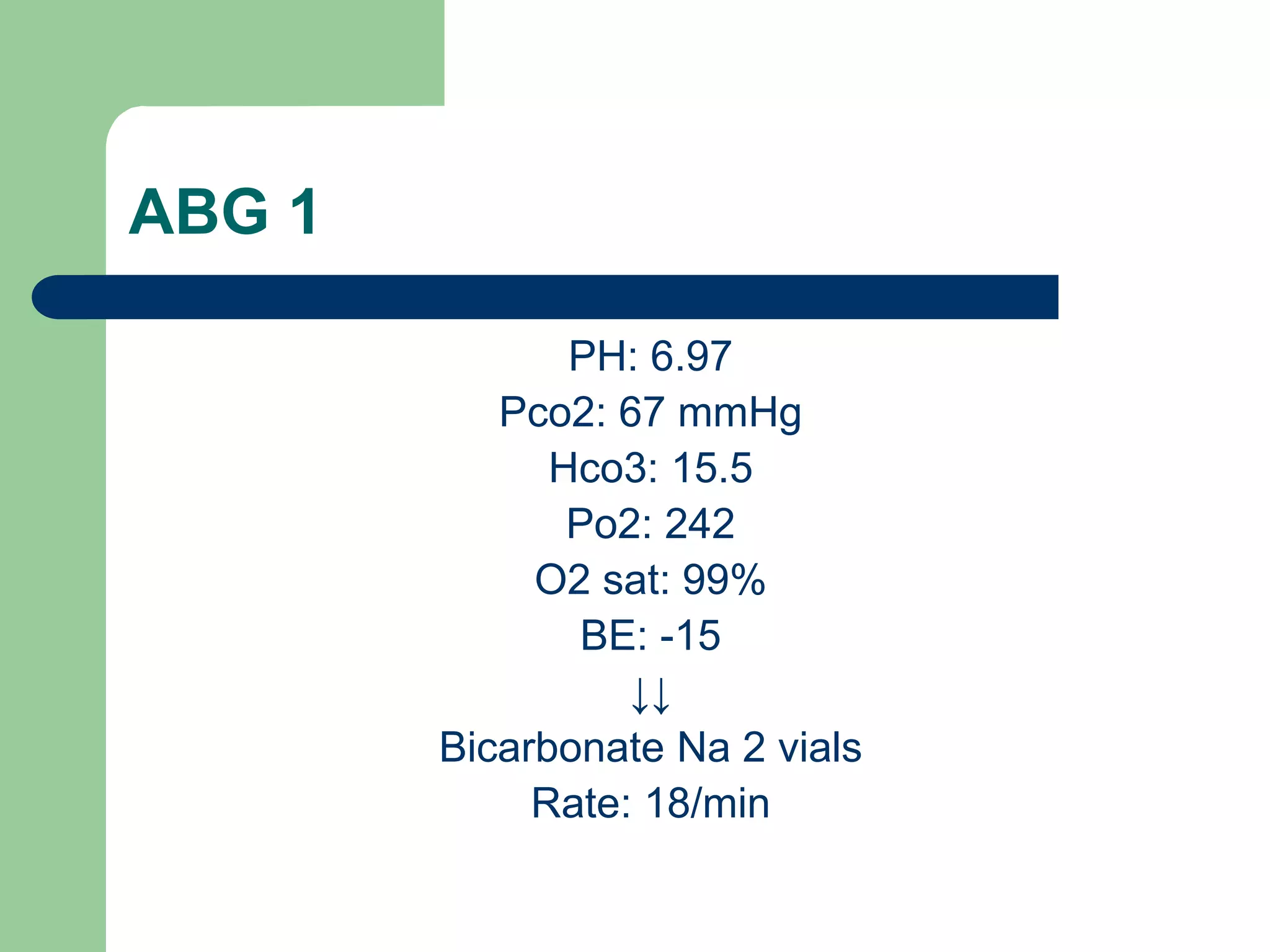
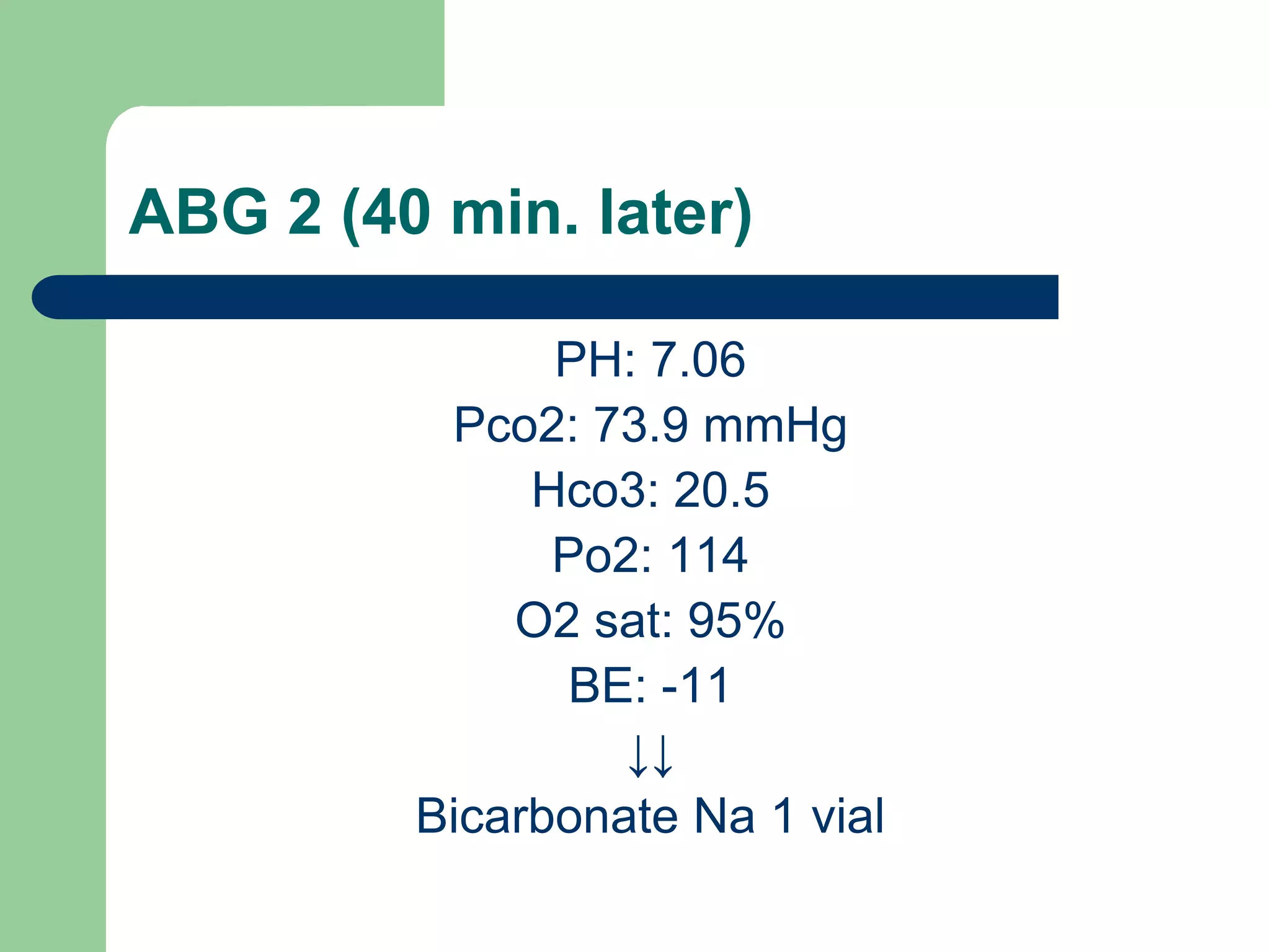













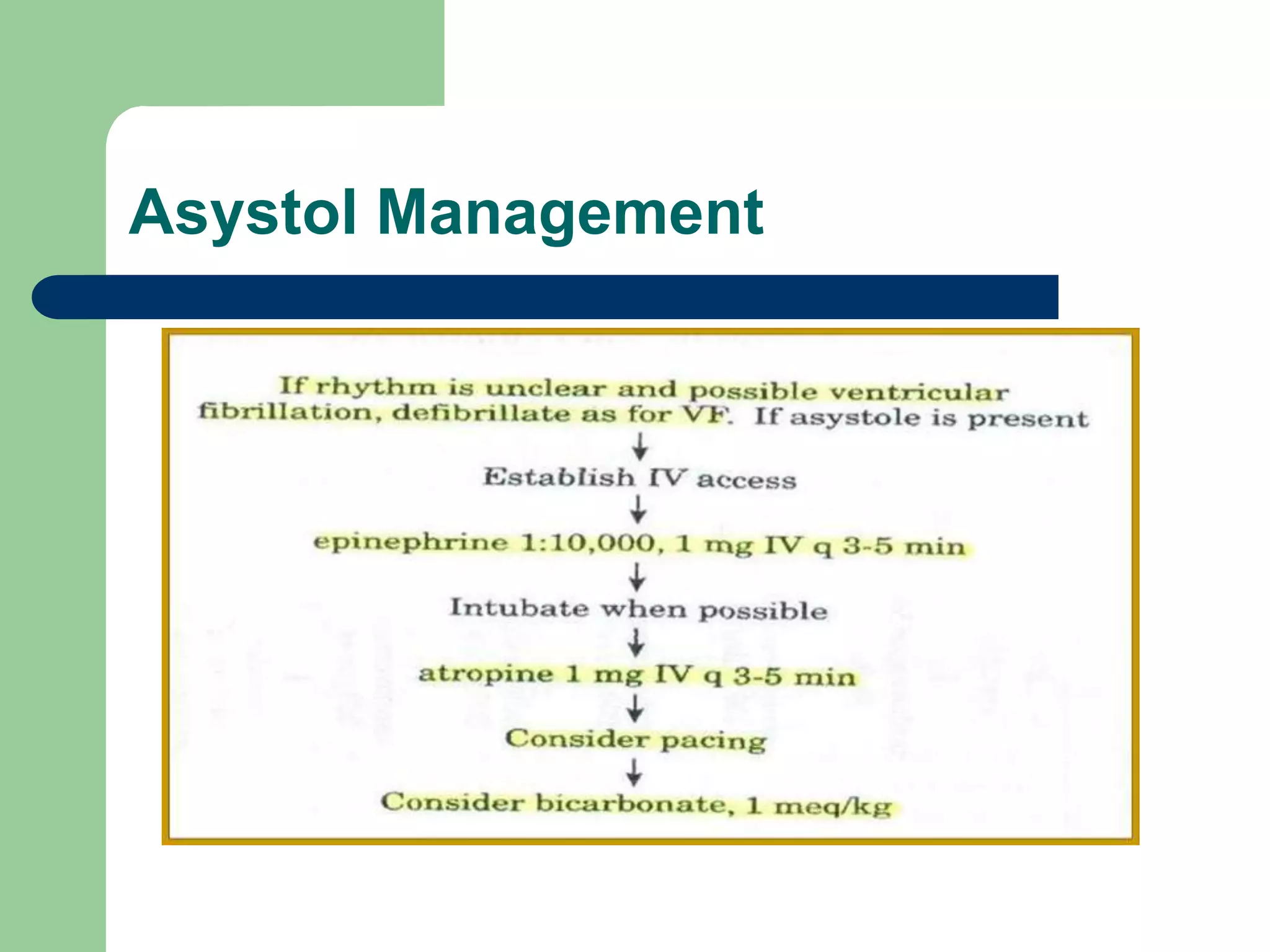



This case report describes the anesthetic management of a patient with severe facial trauma from a car accident. The patient experienced cardiac arrest after induction with fentanyl and propofol. Resuscitation was performed including external cardiac massage, adrenaline, bicarbonate, and lidocaine. Sinus tachycardia was achieved. The patient was found to have pneumothorax requiring chest tube insertion and developing subcutaneous emphysema in the neck requiring surgery. In the ICU, the patient required inotropic support with dobutamine before being weaned. The report concludes with lessons around securing the airway in facial trauma and managing compromised airways.



















































![Approach_to_the_trauma_patient[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/approachtothetraumapatient1-220906191256-c4d92395-thumbnail.jpg?width=640&height=640&fit=bounds)

























