Downloaded 18 times


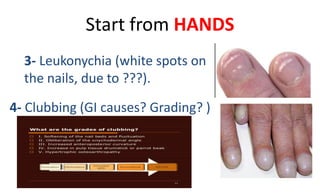

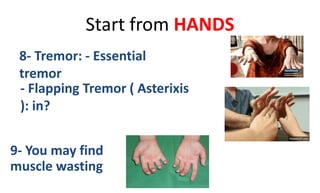

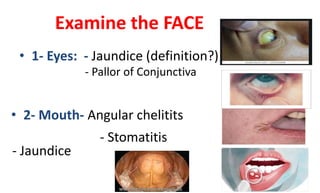
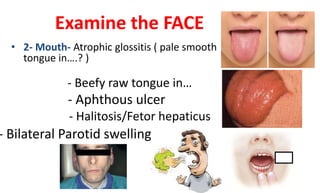




The document outlines a comprehensive guide for conducting a gastrointestinal examination by Dr. Anas Aljundi, emphasizing the importance of initial interactions, patient appearance, vital signs, and specific examination techniques. It details steps for assessing the hands, face, thorax, and abdomen, including inspection, palpation, and auscultation for various conditions like hepatomegaly and splenomegaly. The protocol concludes with guidelines for examining the groin, external genitalia, lymph nodes, anal area, and lower limbs.

![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)

































































