Downloaded 2,166 times





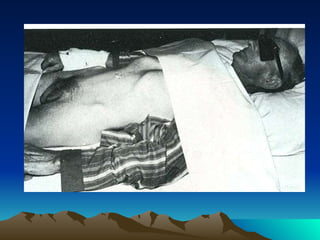



















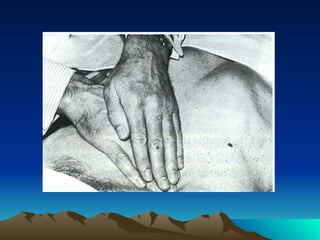












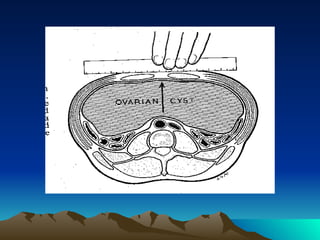










































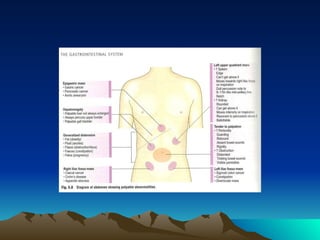




The document provides guidance on performing an abdominal examination, including inspection, palpation, percussion, and auscultation of the abdomen. It describes how to examine the liver, spleen, kidneys, abdominal aorta, hernias and abdominal masses. Key steps include systematic inspection for abnormalities, deep and superficial palpation using both hands, percussion to determine dullness and resonance, and auscultation of bowel sounds and vascular bruits. Practice is emphasized to gain skill in abdominal examination techniques.







![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)



























































