Downloaded 83 times





























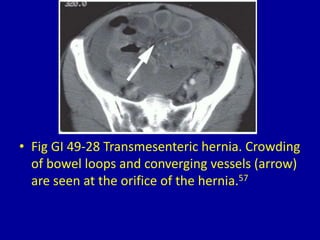











This document contains 34 figures showing various abdominal hernias as seen on imaging studies like CT scans and barium studies. It describes different types of hernias including paraduodenal, inguinal, femoral, umbilical, incisional, lumbar, and transmesenteric hernias. The images demonstrate the location and contents of the hernia sacs as well as complications like strangulation or obstruction.































































































