Downloaded 13 times
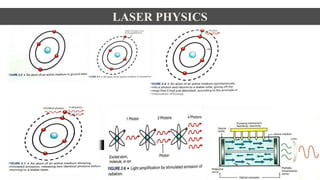
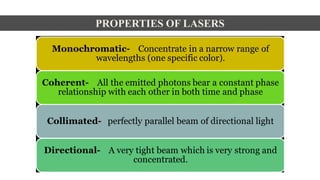
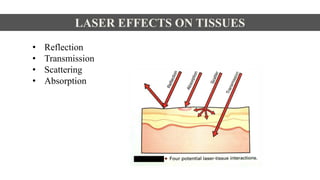

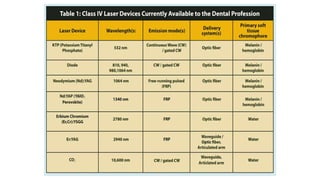
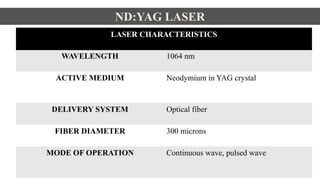
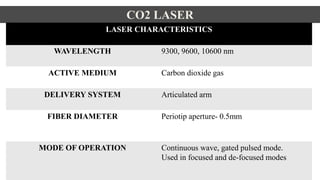
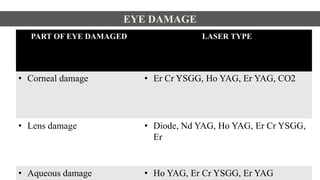

This document discusses lasers used in periodontics. It provides an overview of laser physics, types of lasers including diode, CO2, Nd:YAG and erbium lasers, and their applications in soft tissue procedures and osseous surgery. The benefits of lasers include less pain, better hemostasis and wound healing compared to conventional methods. Safety protocols must be followed when using lasers to prevent eye and tissue damage. Lasers are becoming more widely used in dentistry due to their advantages over traditional techniques.













































![Laser basics[26239].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/laserbasics26239-231026124741-3b010082-thumbnail.jpg?width=640&height=640&fit=bounds)























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















