The document discusses the anatomic and physiologic differences between pediatric and adult patients that influence anesthetic techniques. Key distinctions include variations in airway structure, respiratory physiology, and cardiovascular function, as well as considerations for preoperative evaluation and anesthetic agents used in children. It emphasizes the importance of understanding these factors for safe and effective pediatric anesthesia practice.

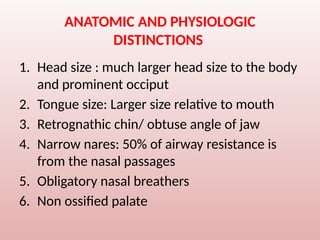
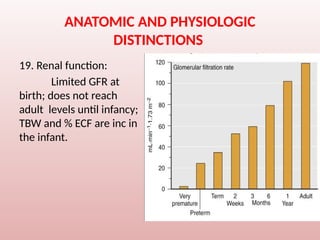
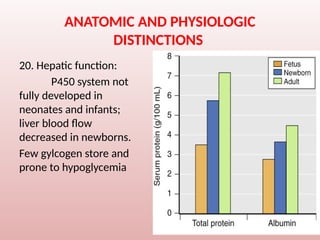





























































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





