Downloaded 64 times
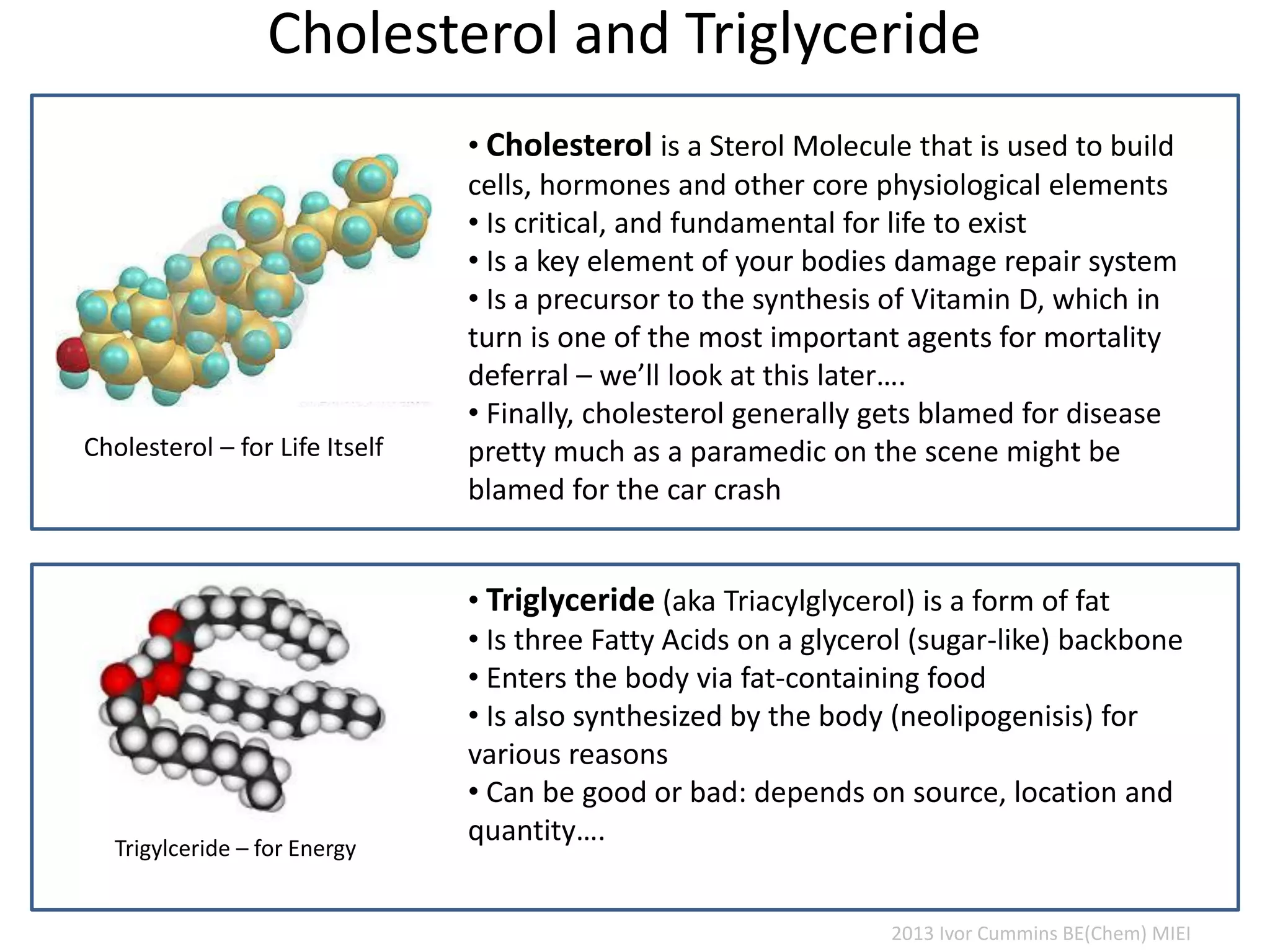
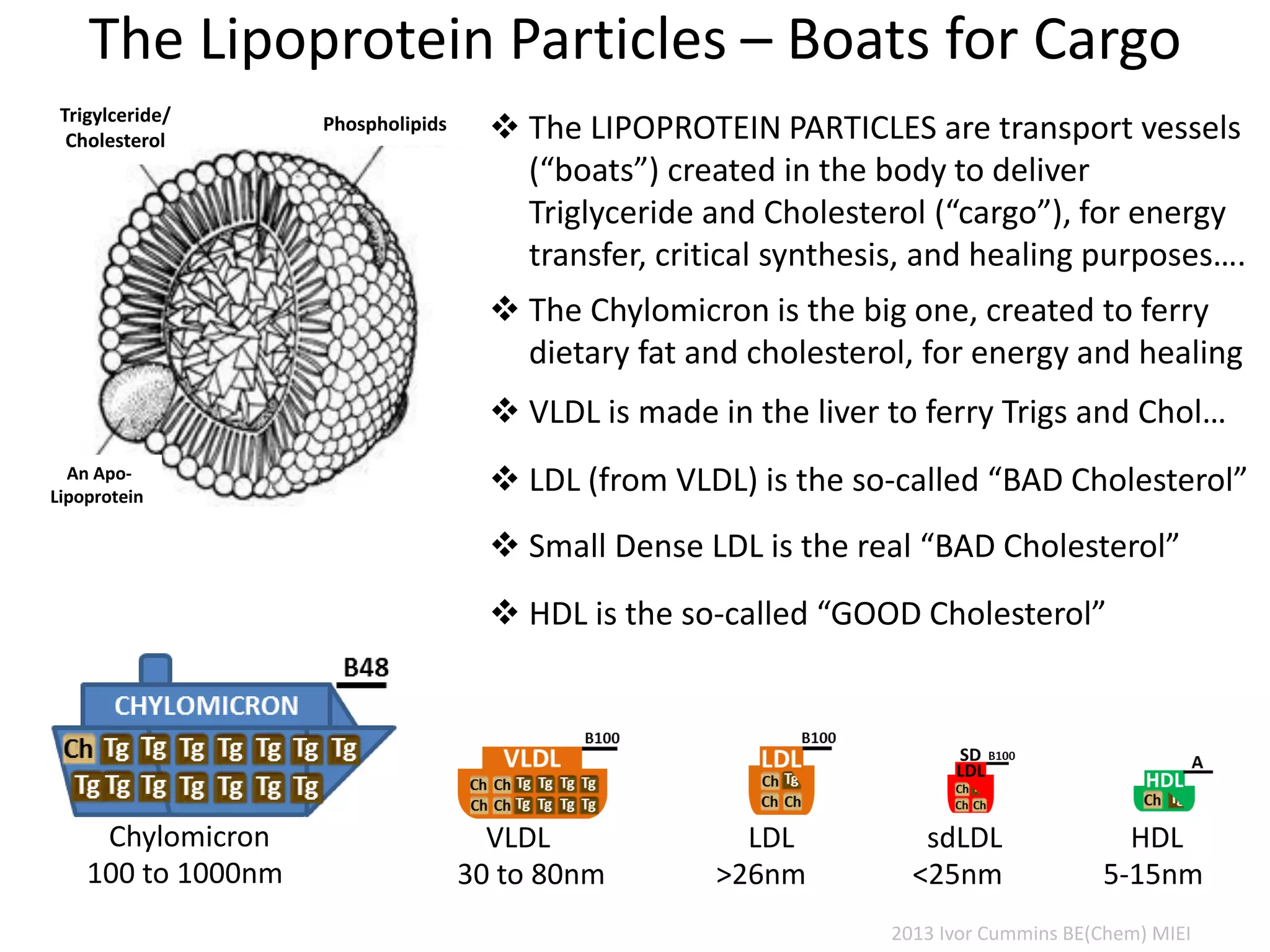

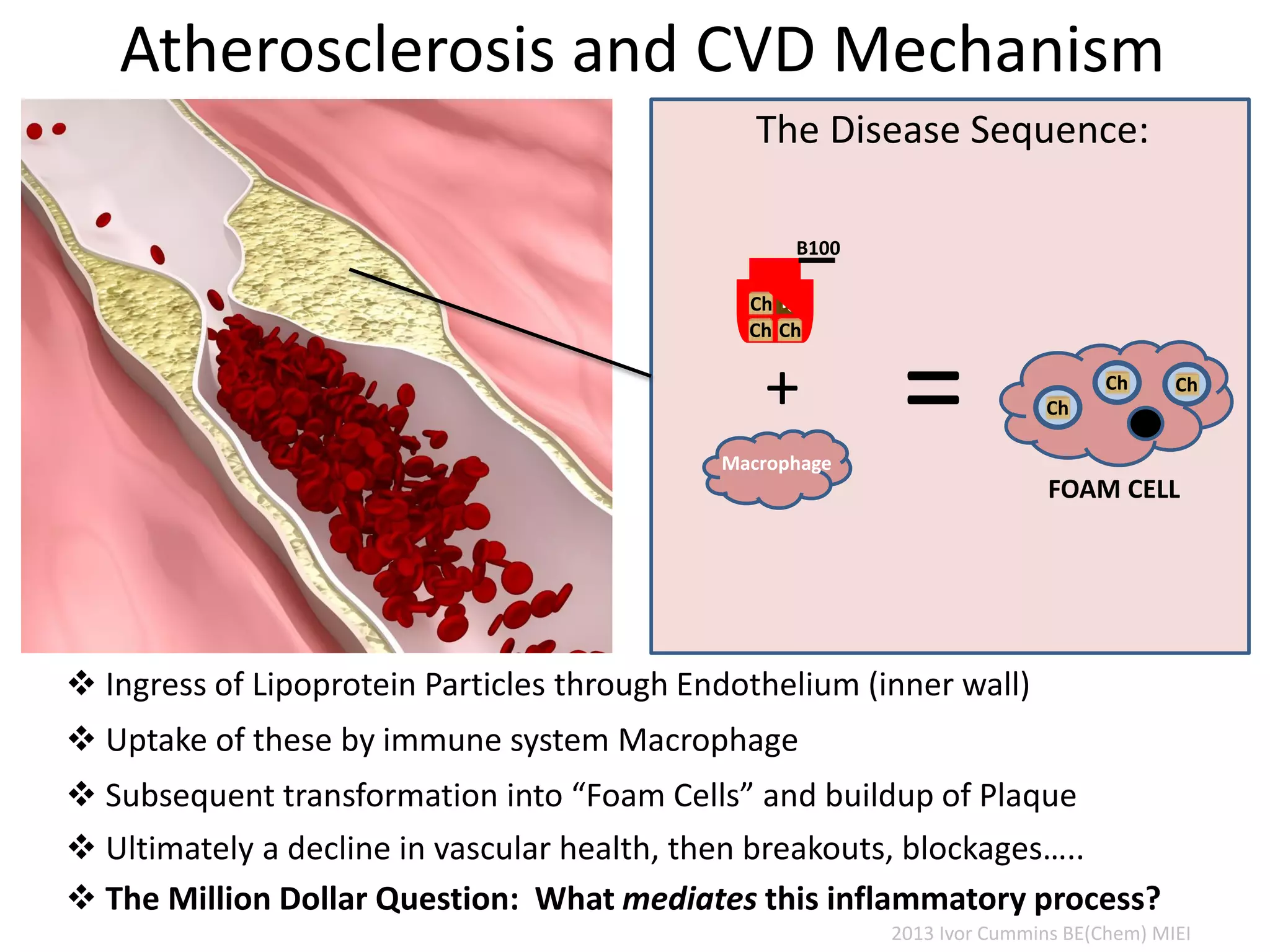
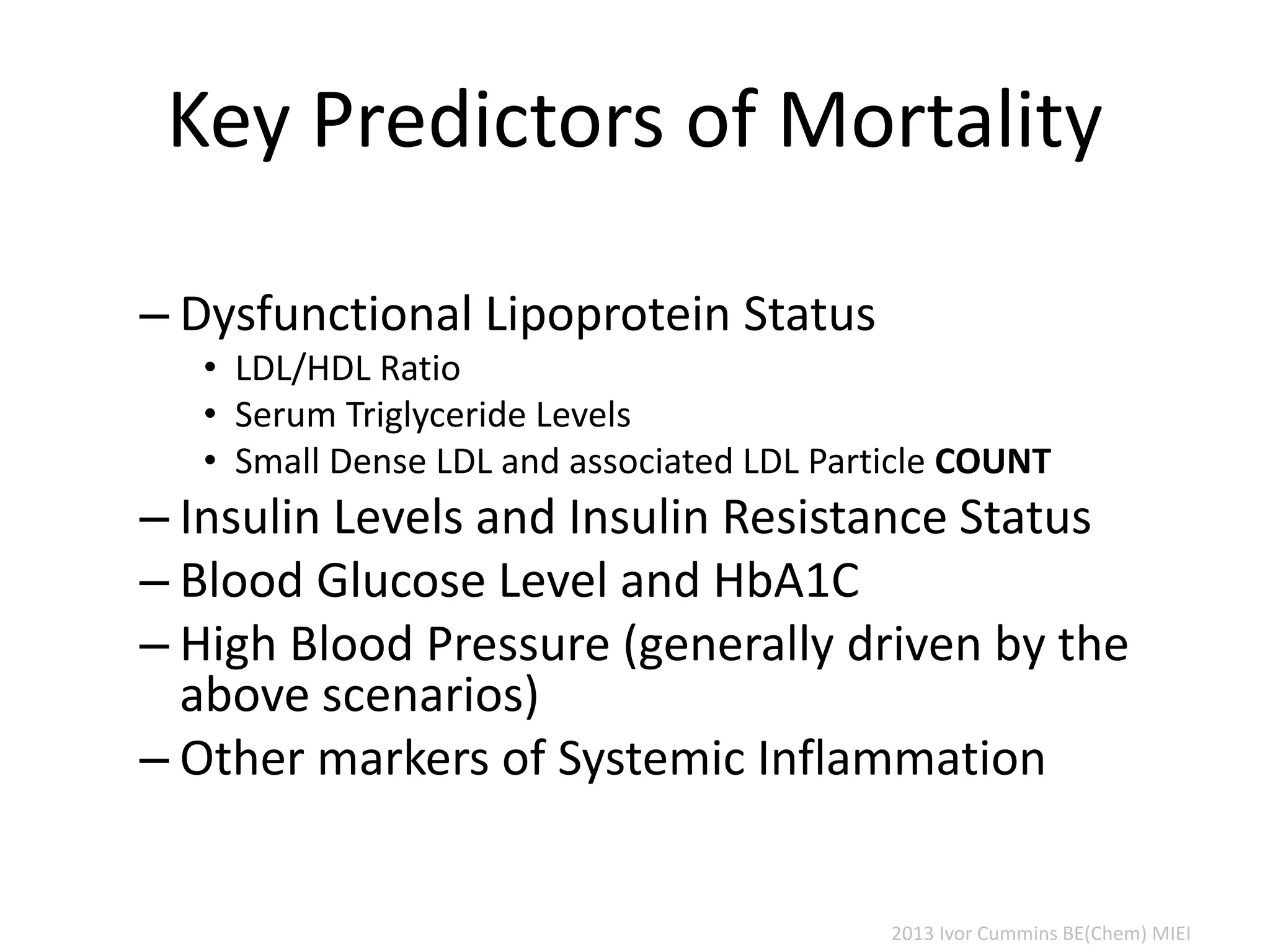
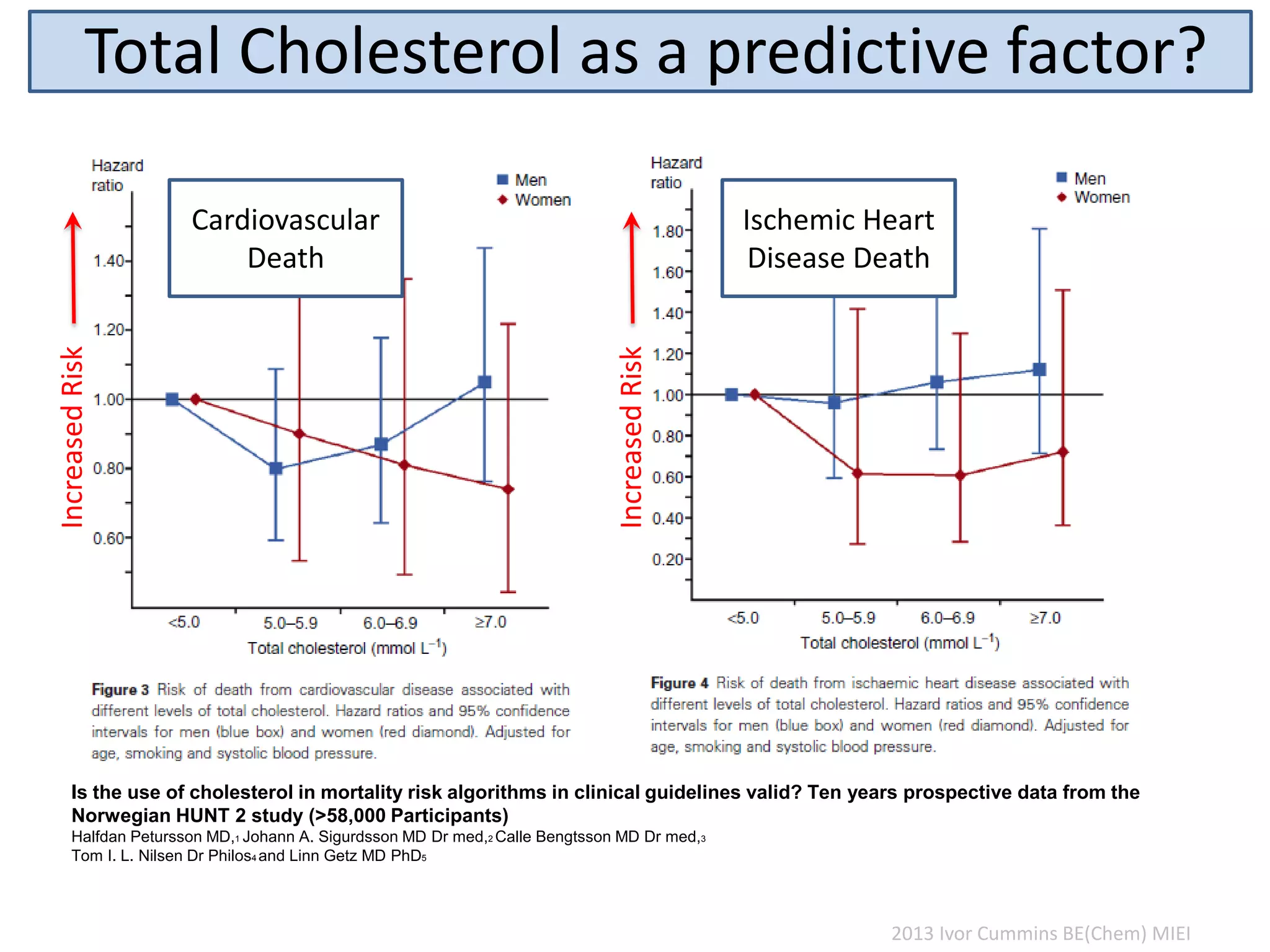
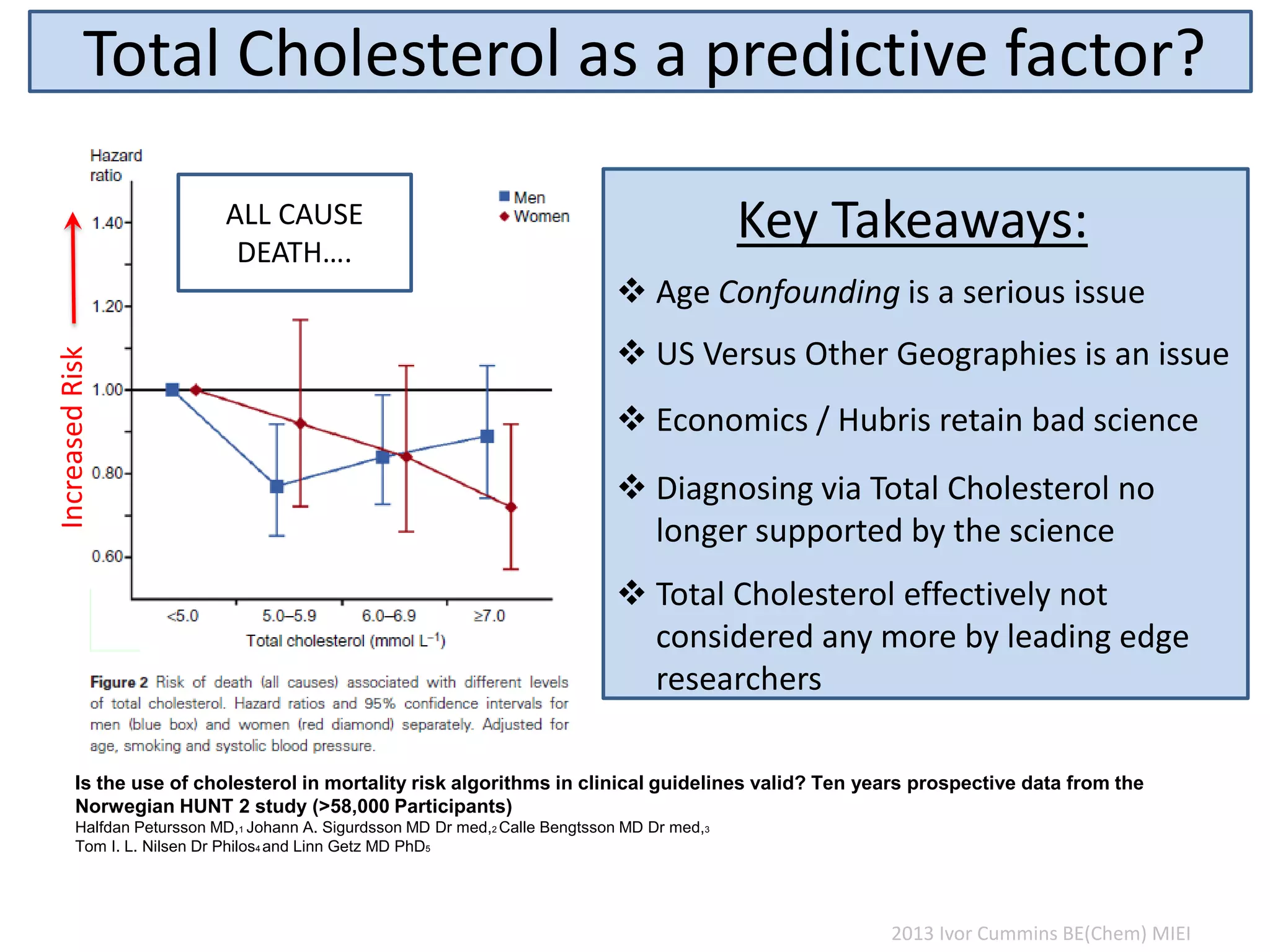
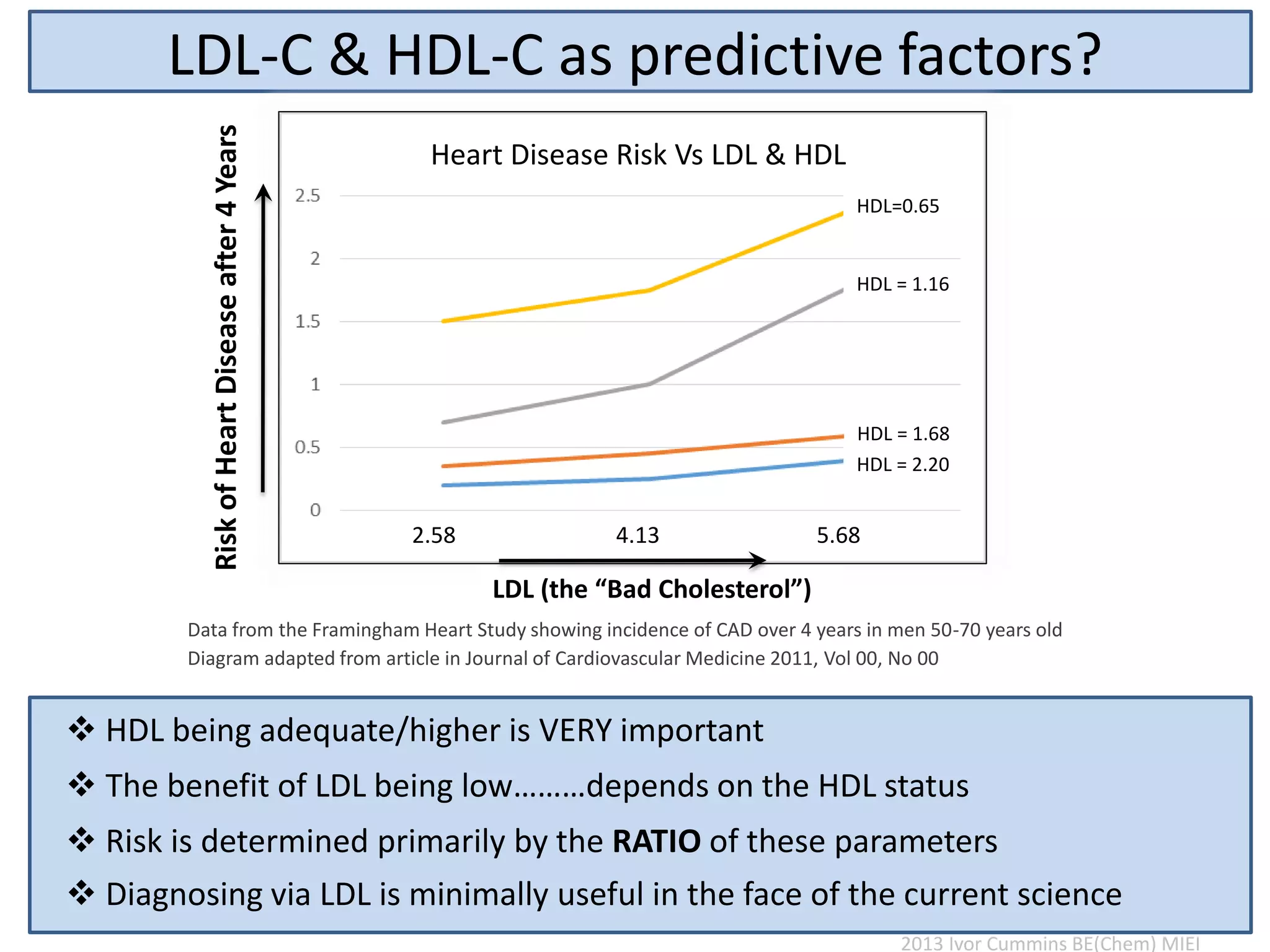
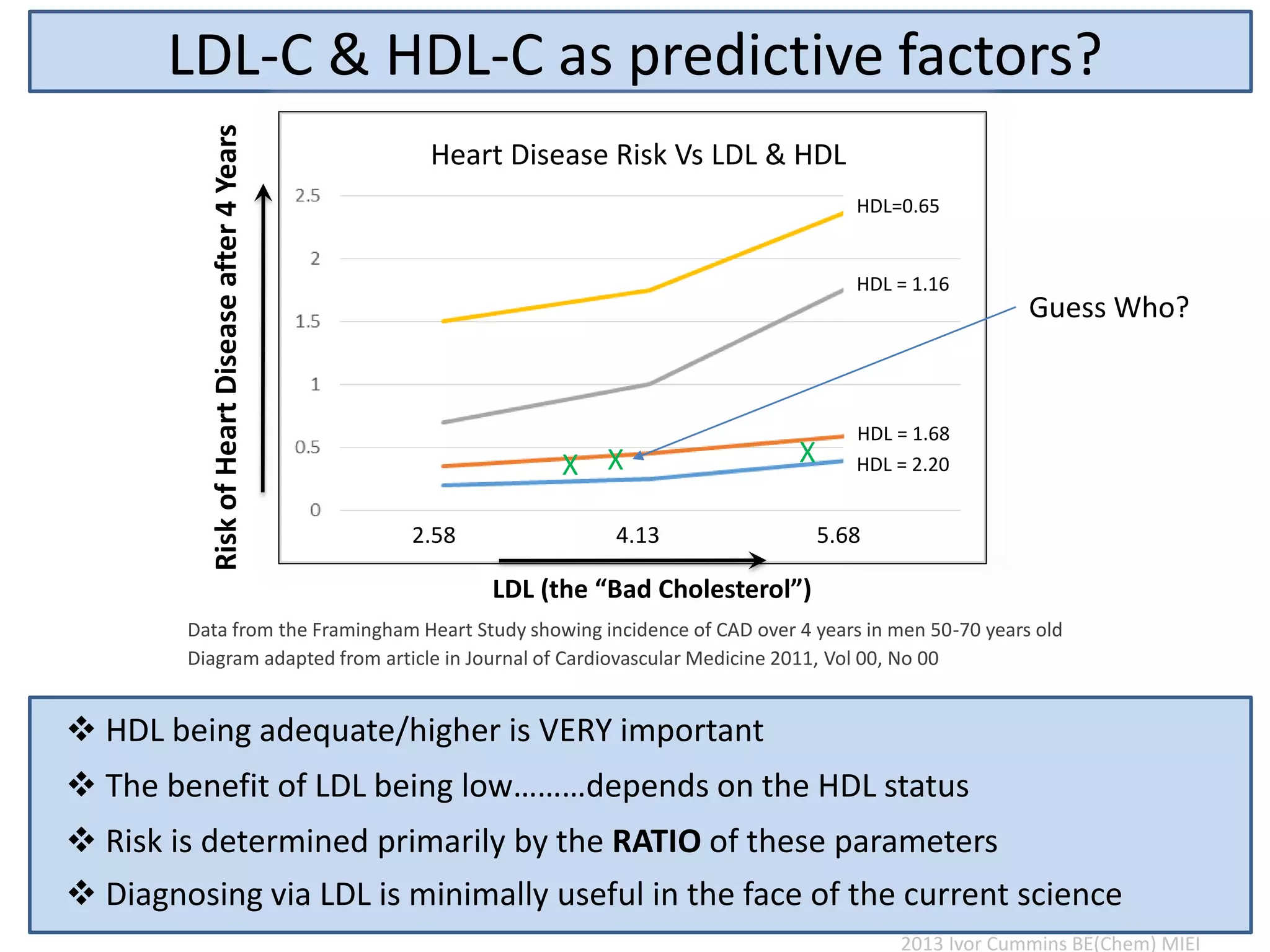

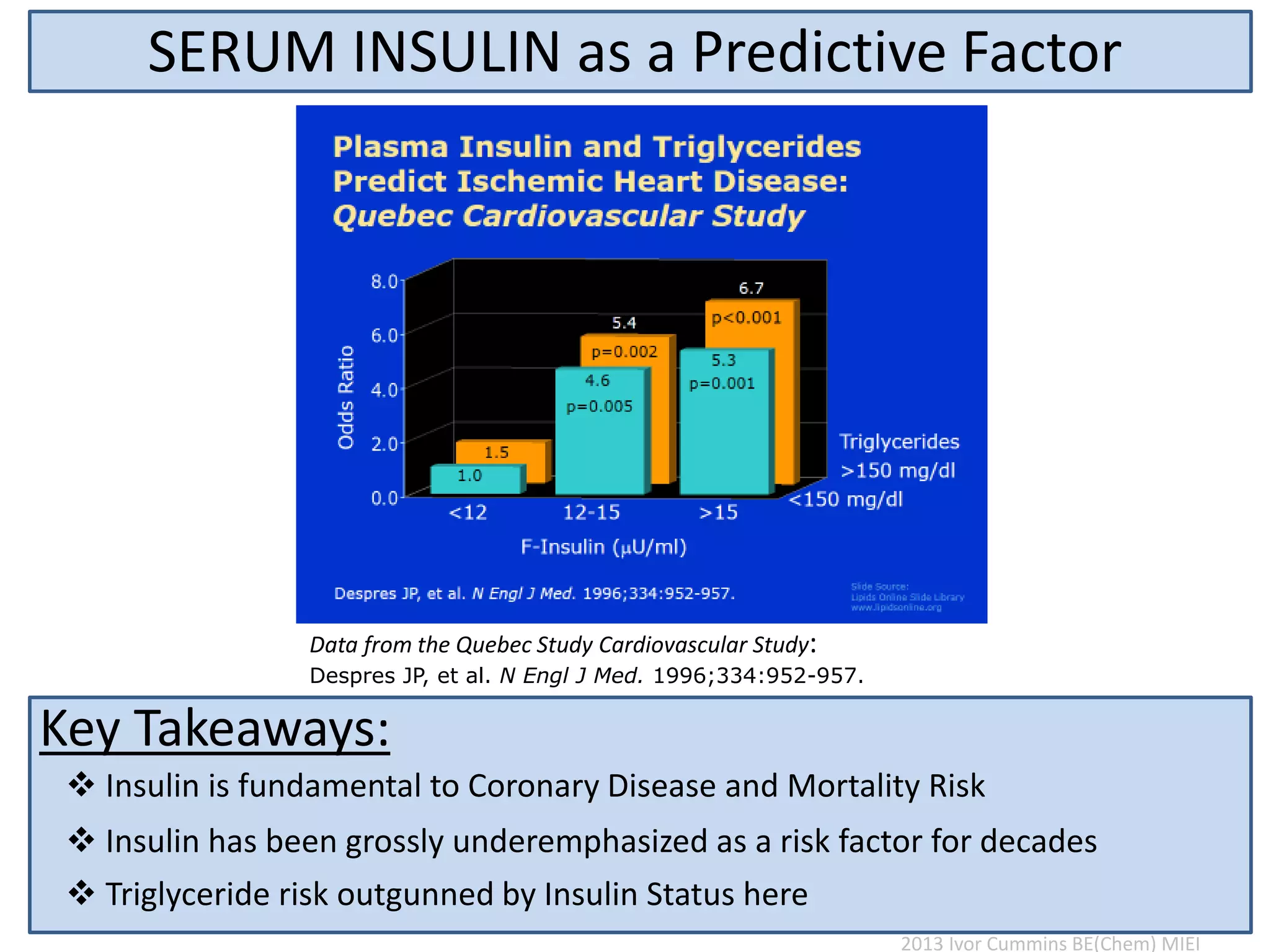
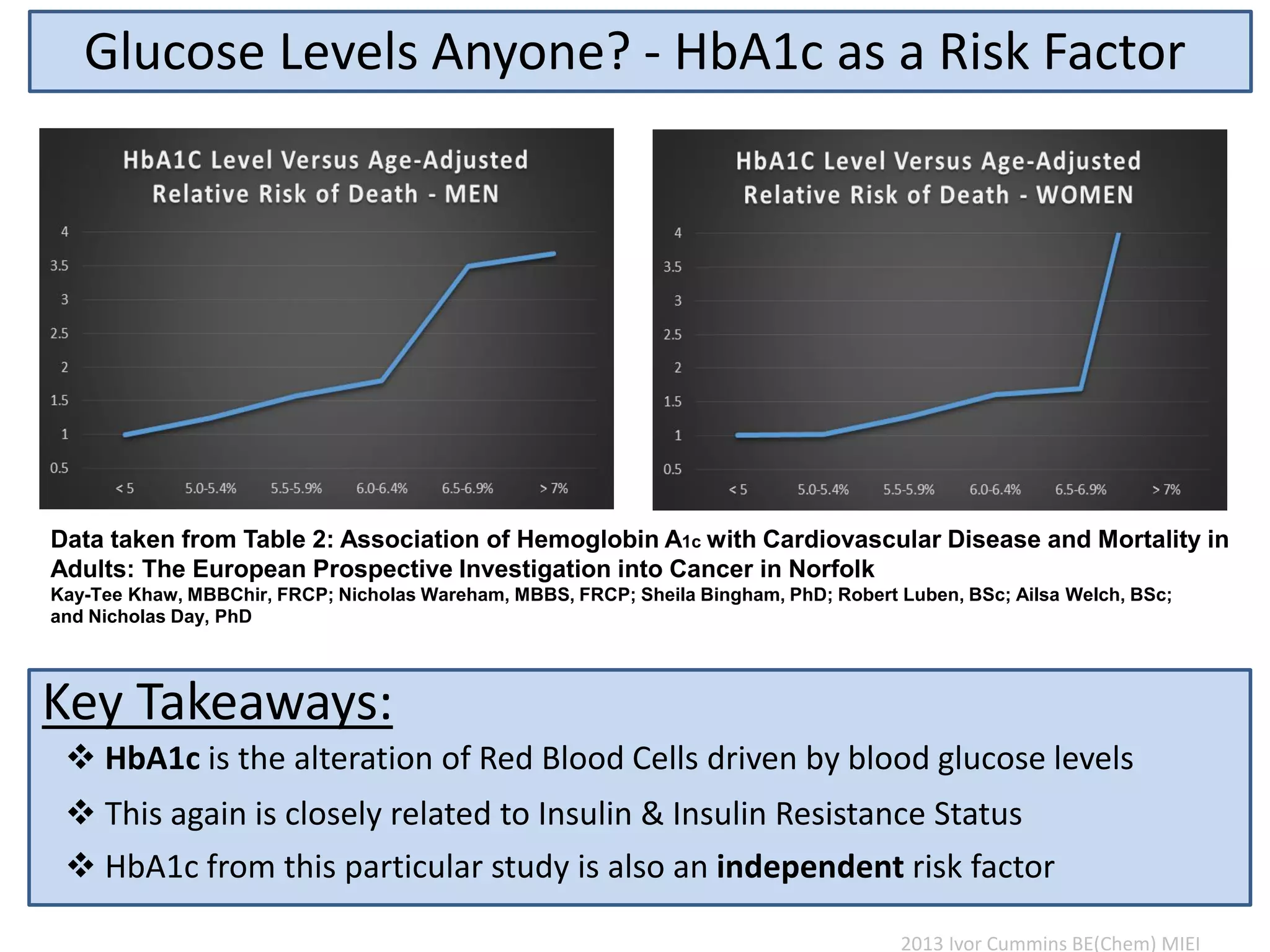
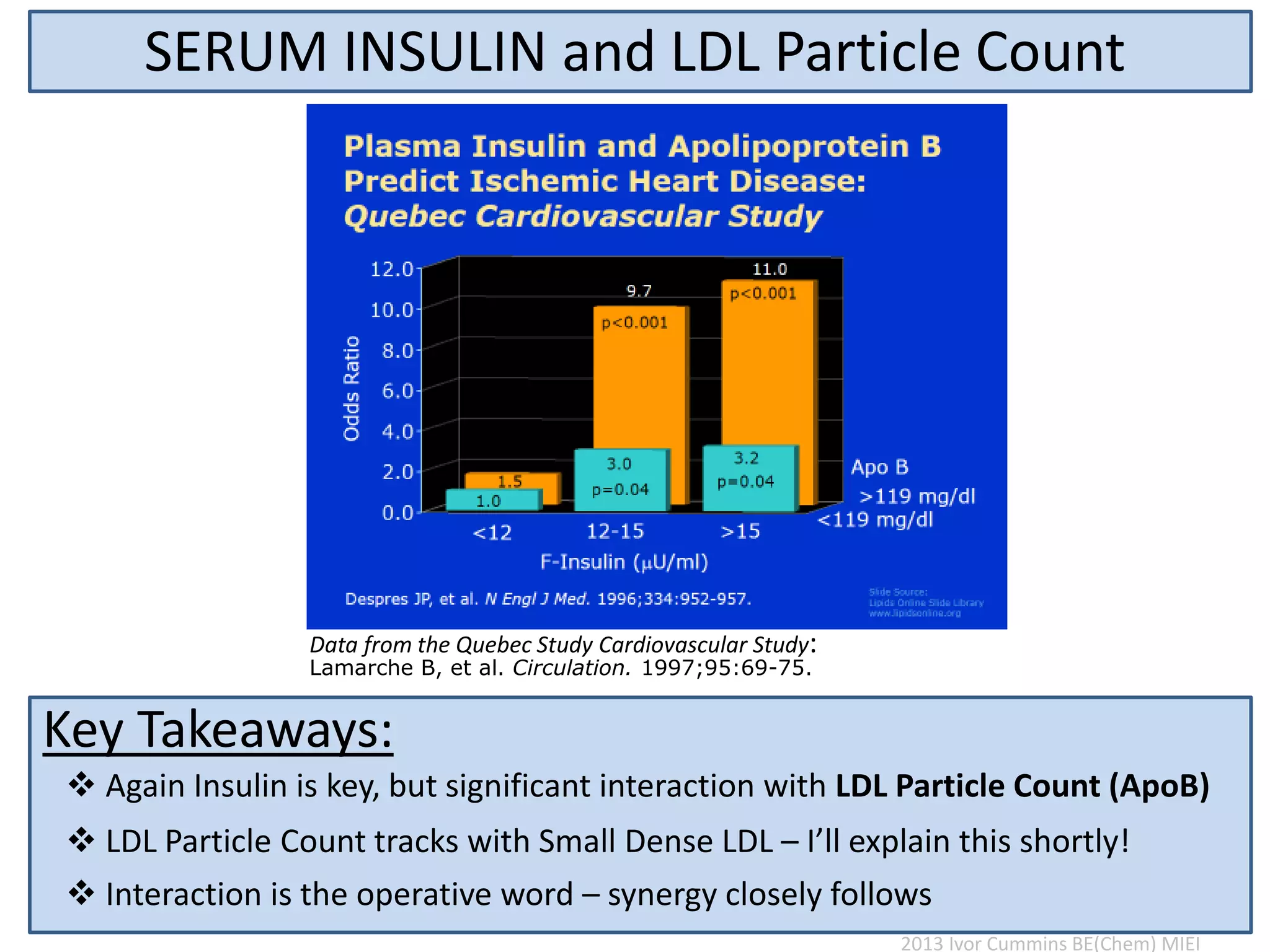
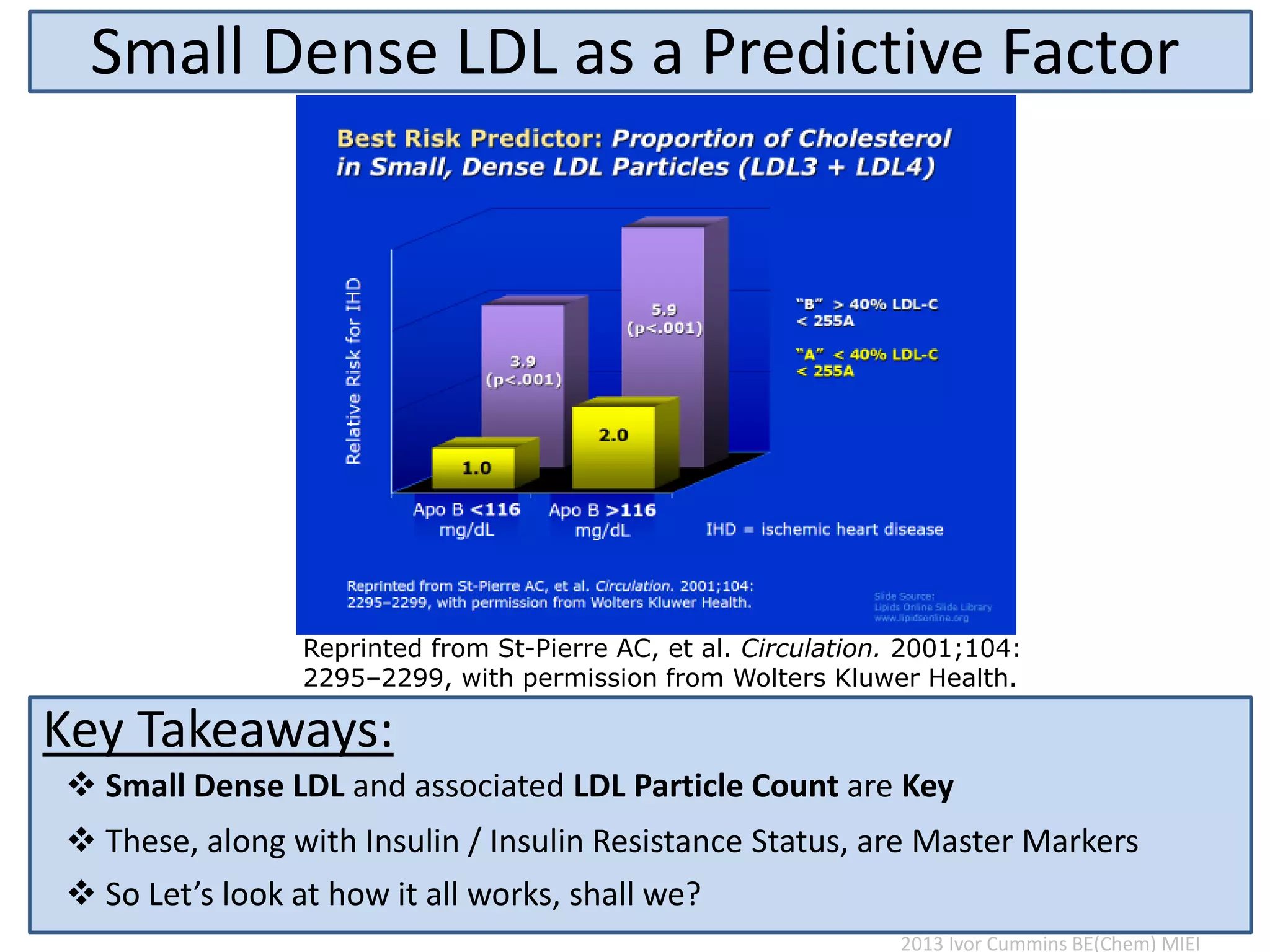
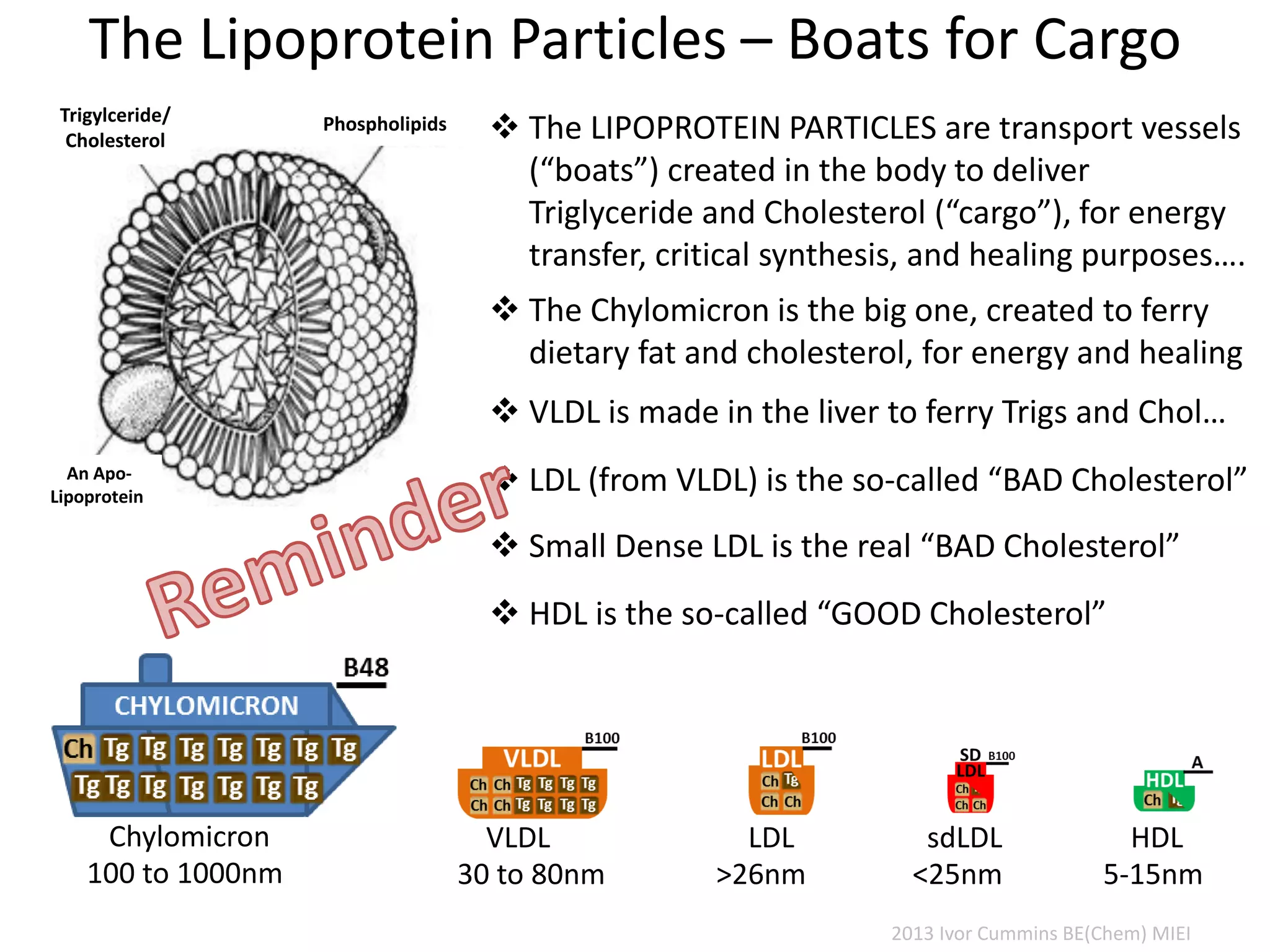
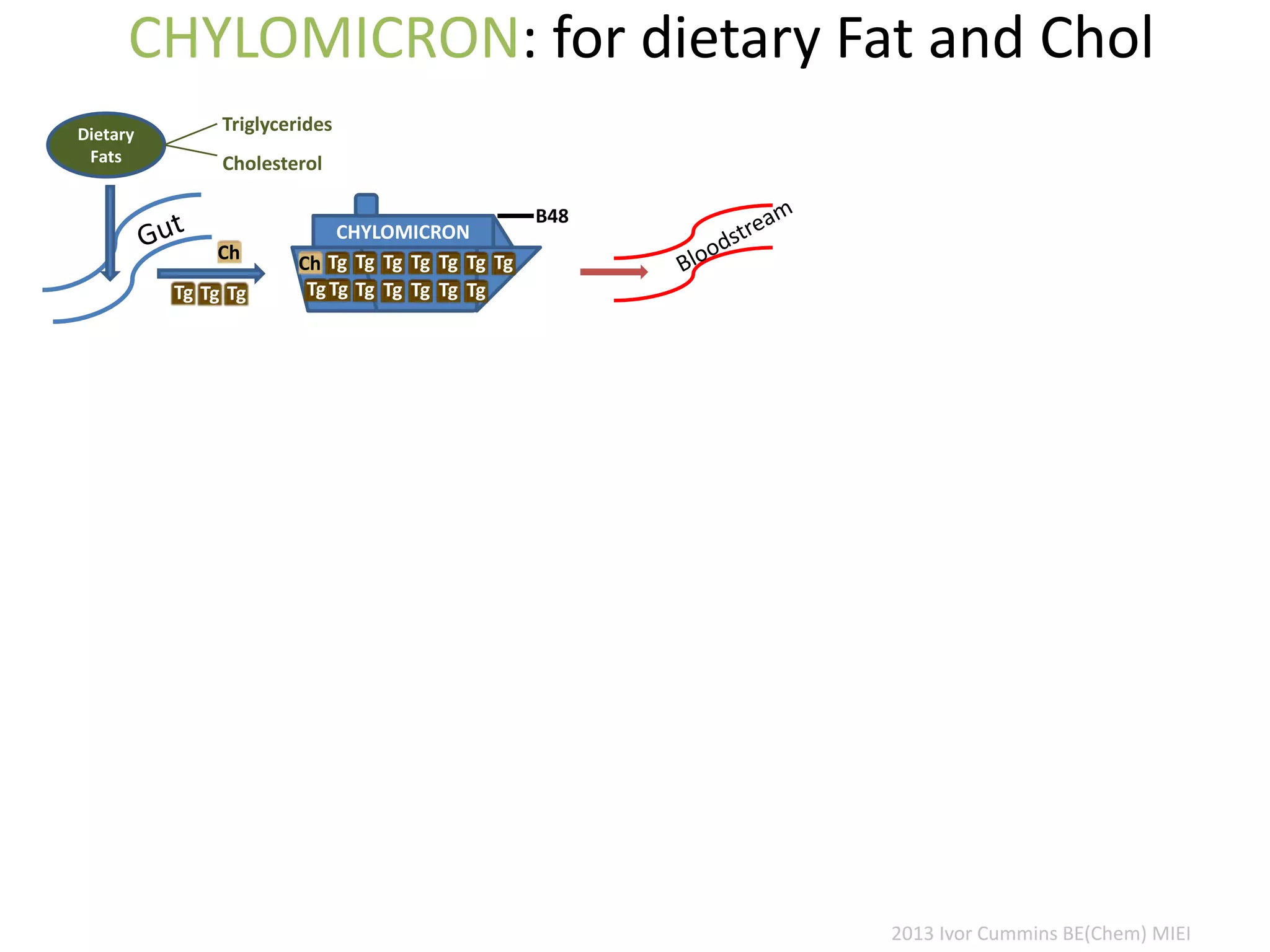
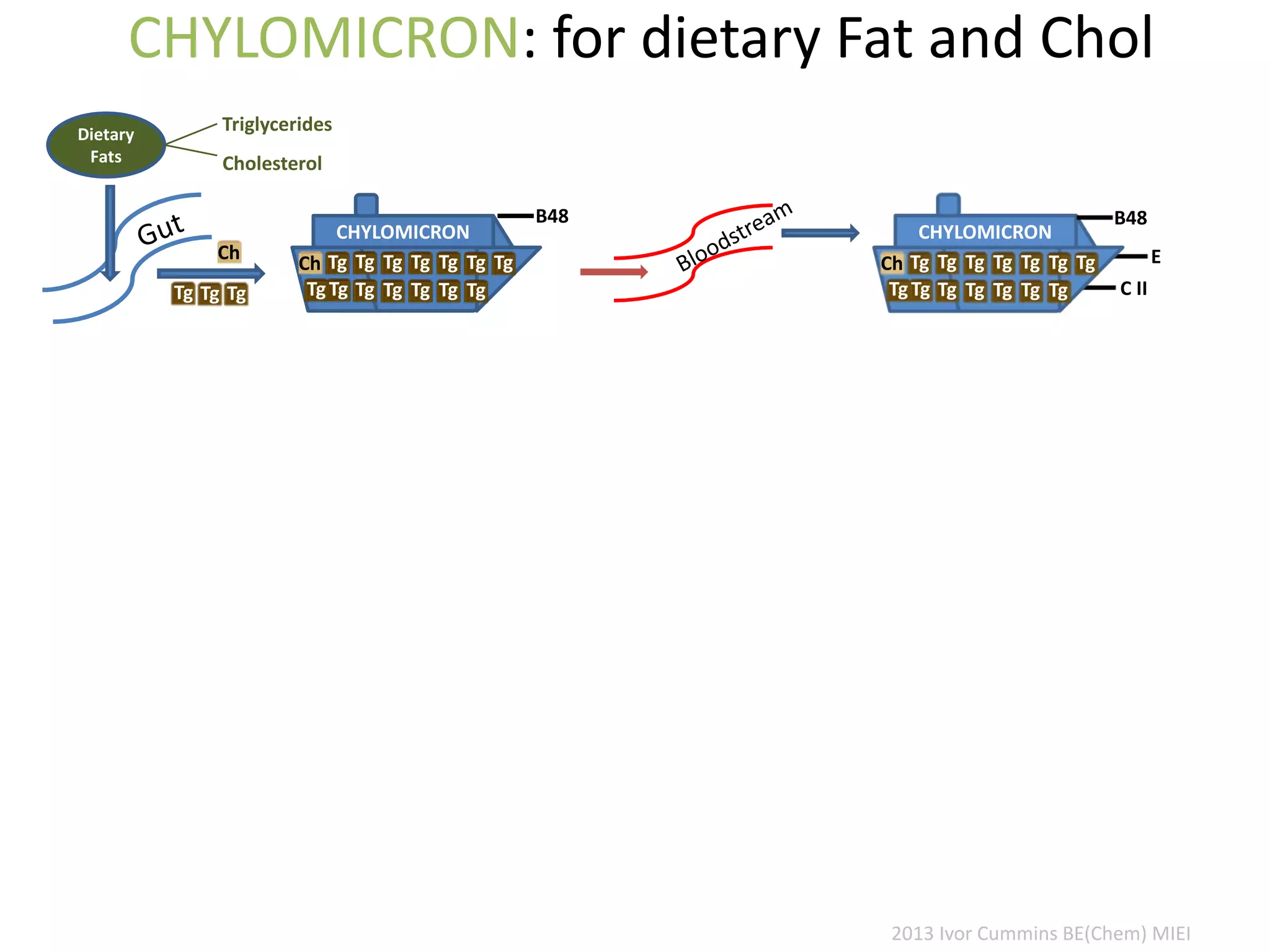

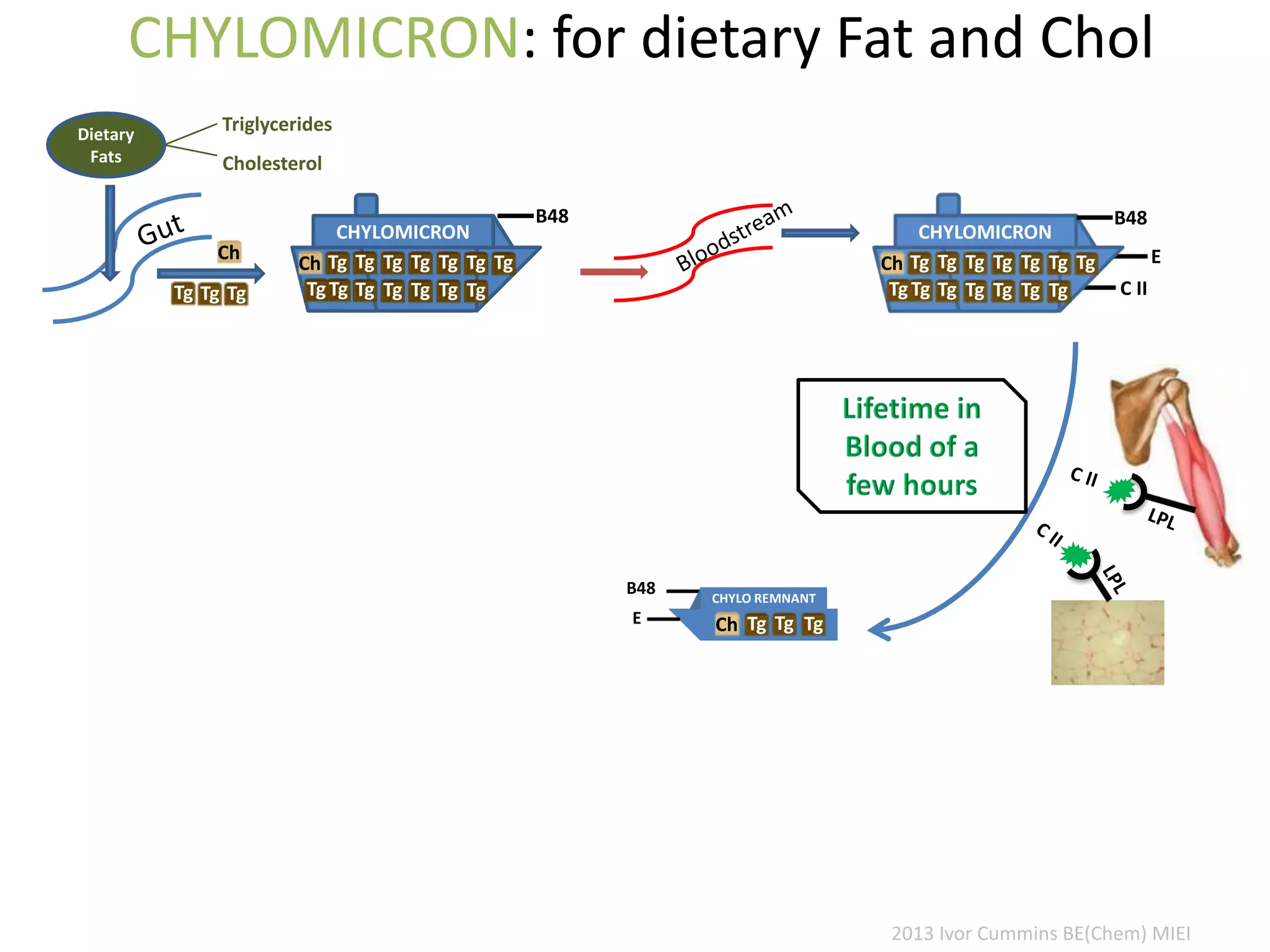
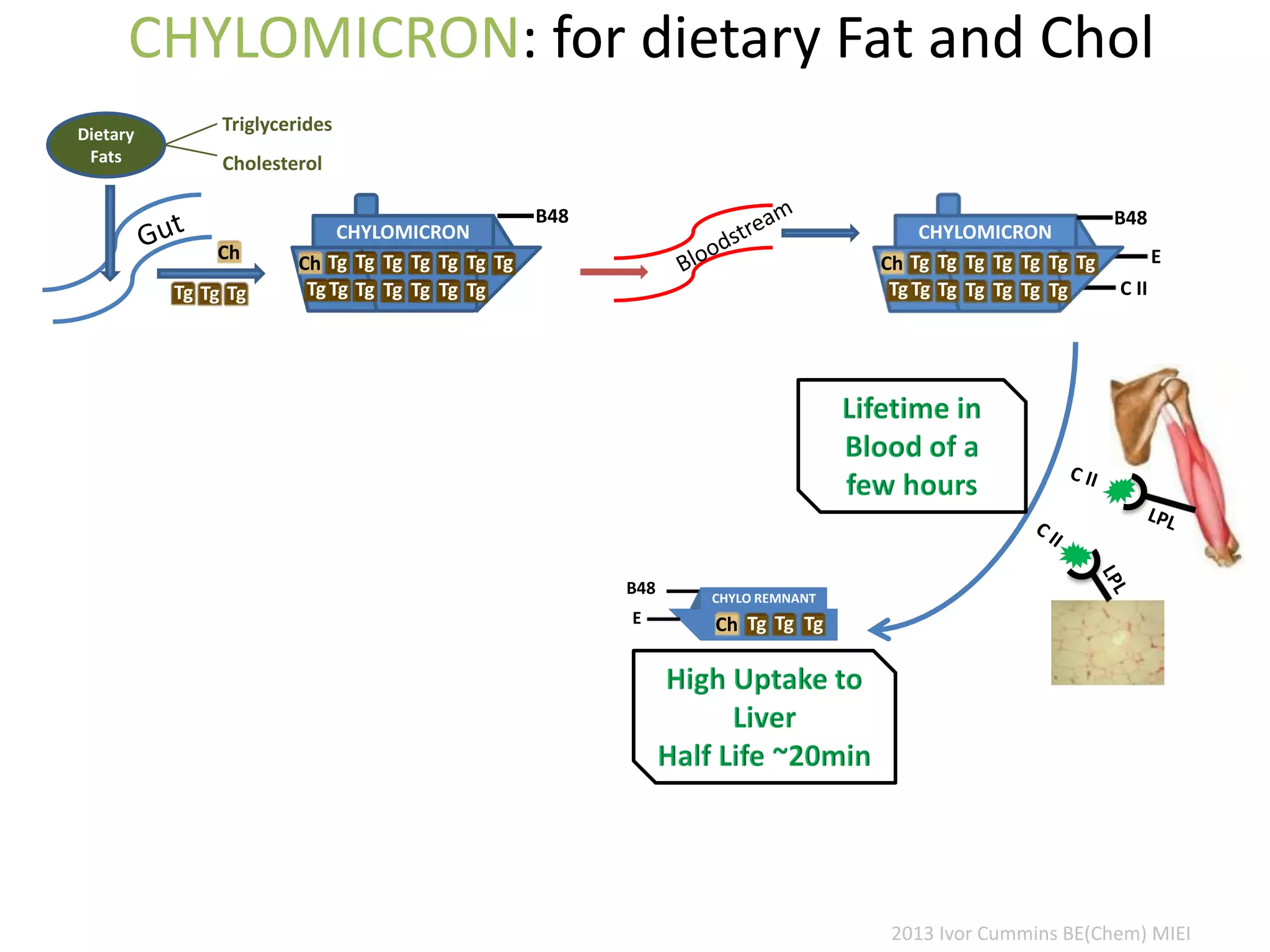
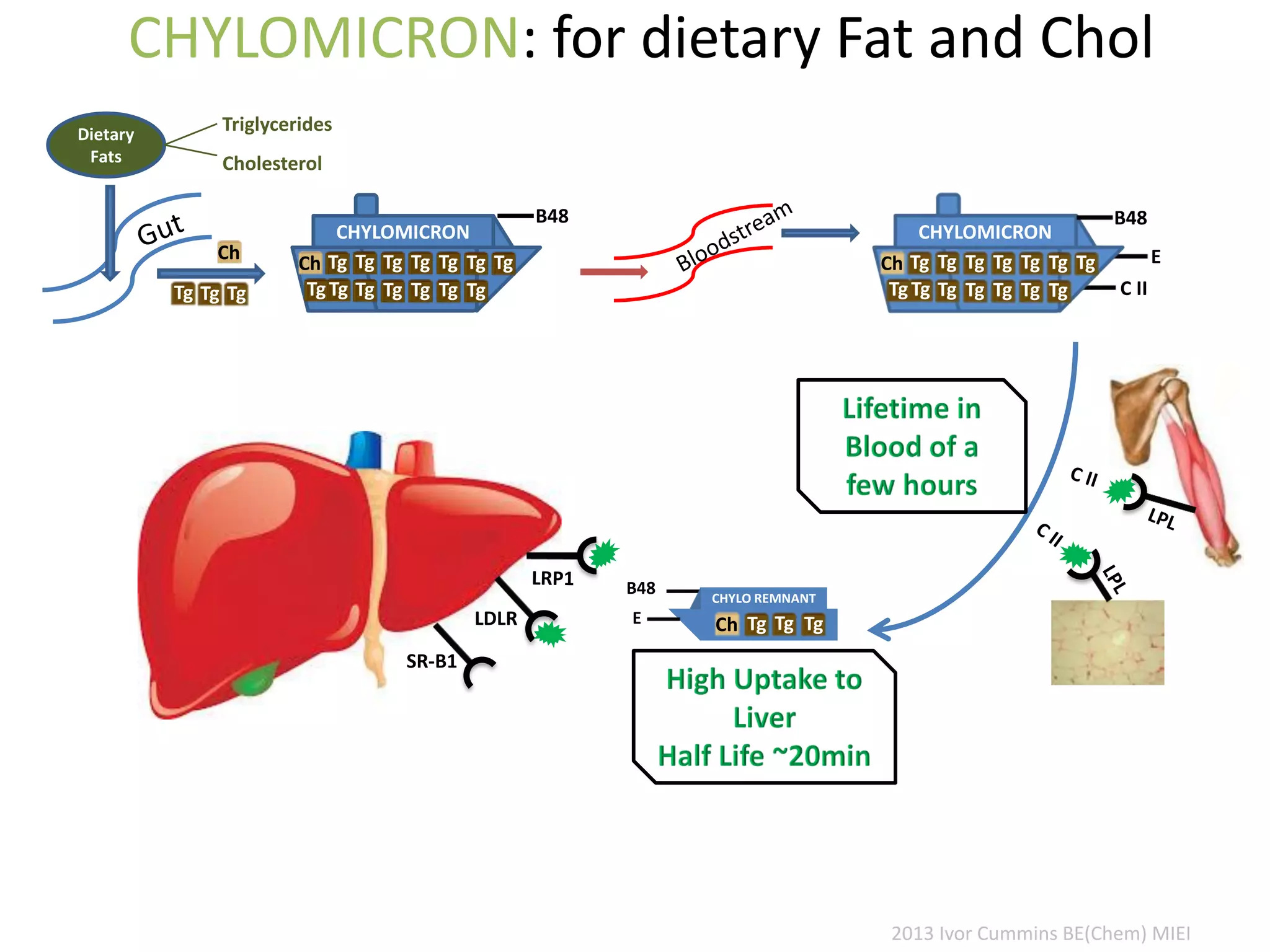
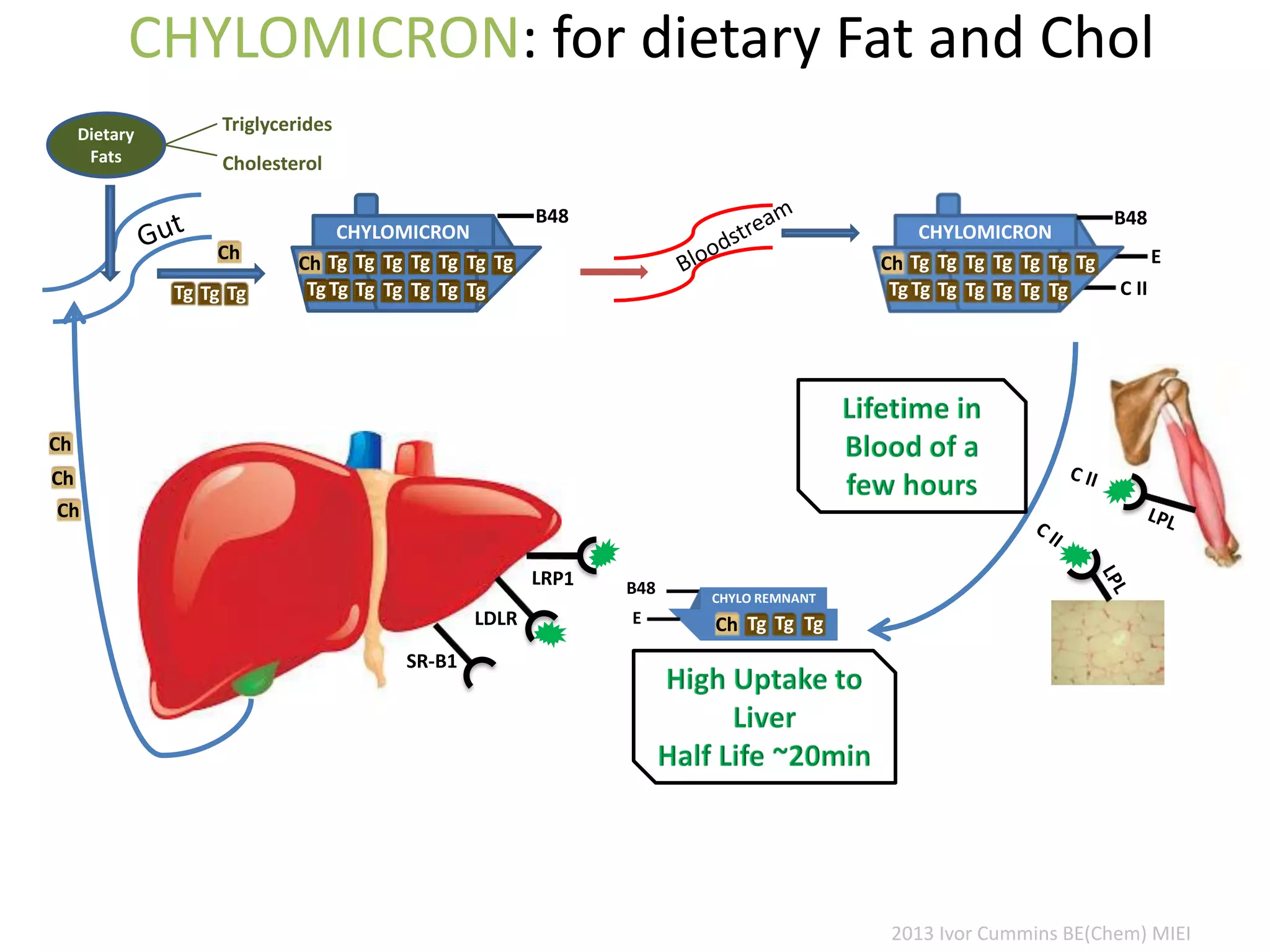
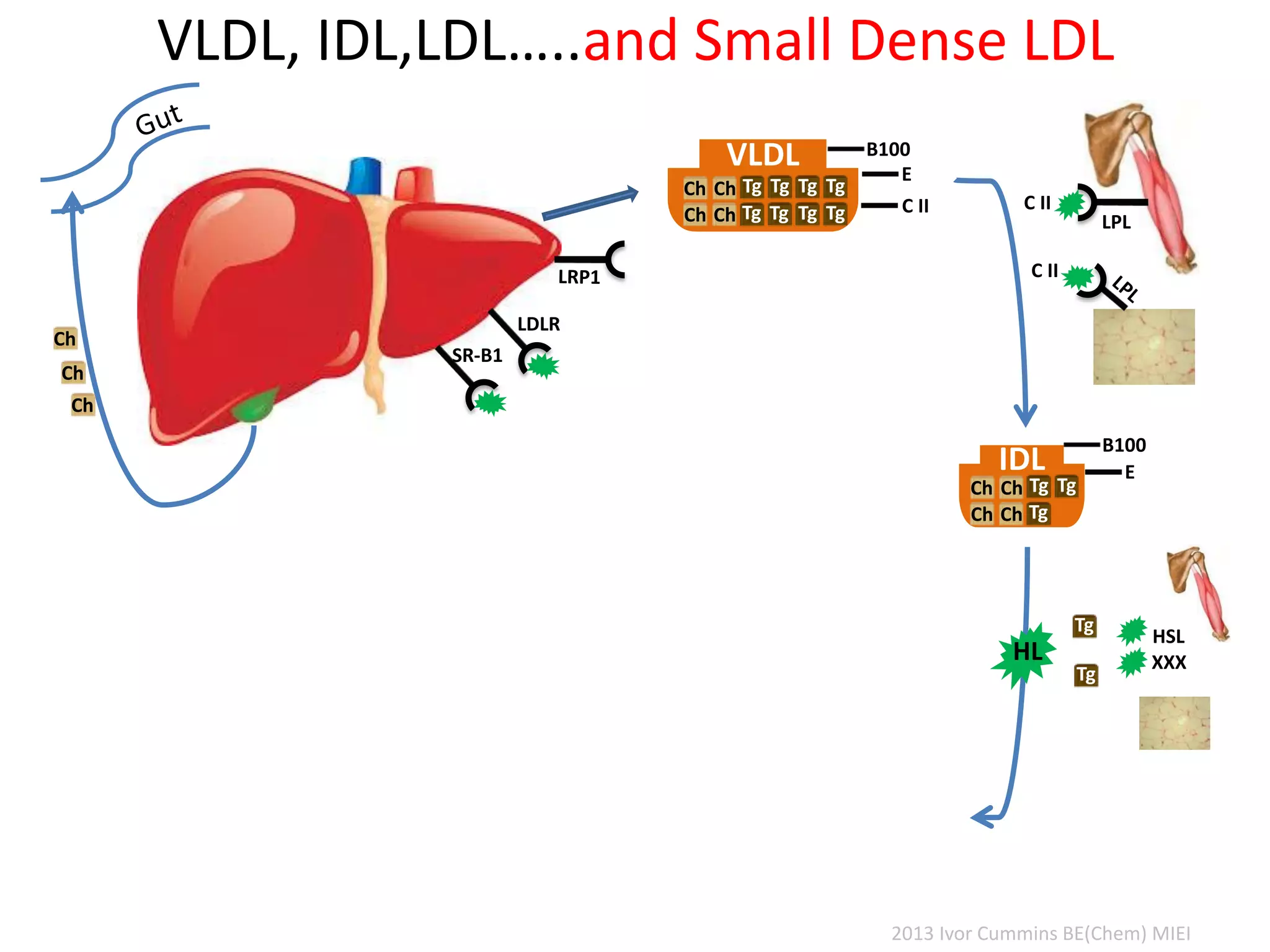
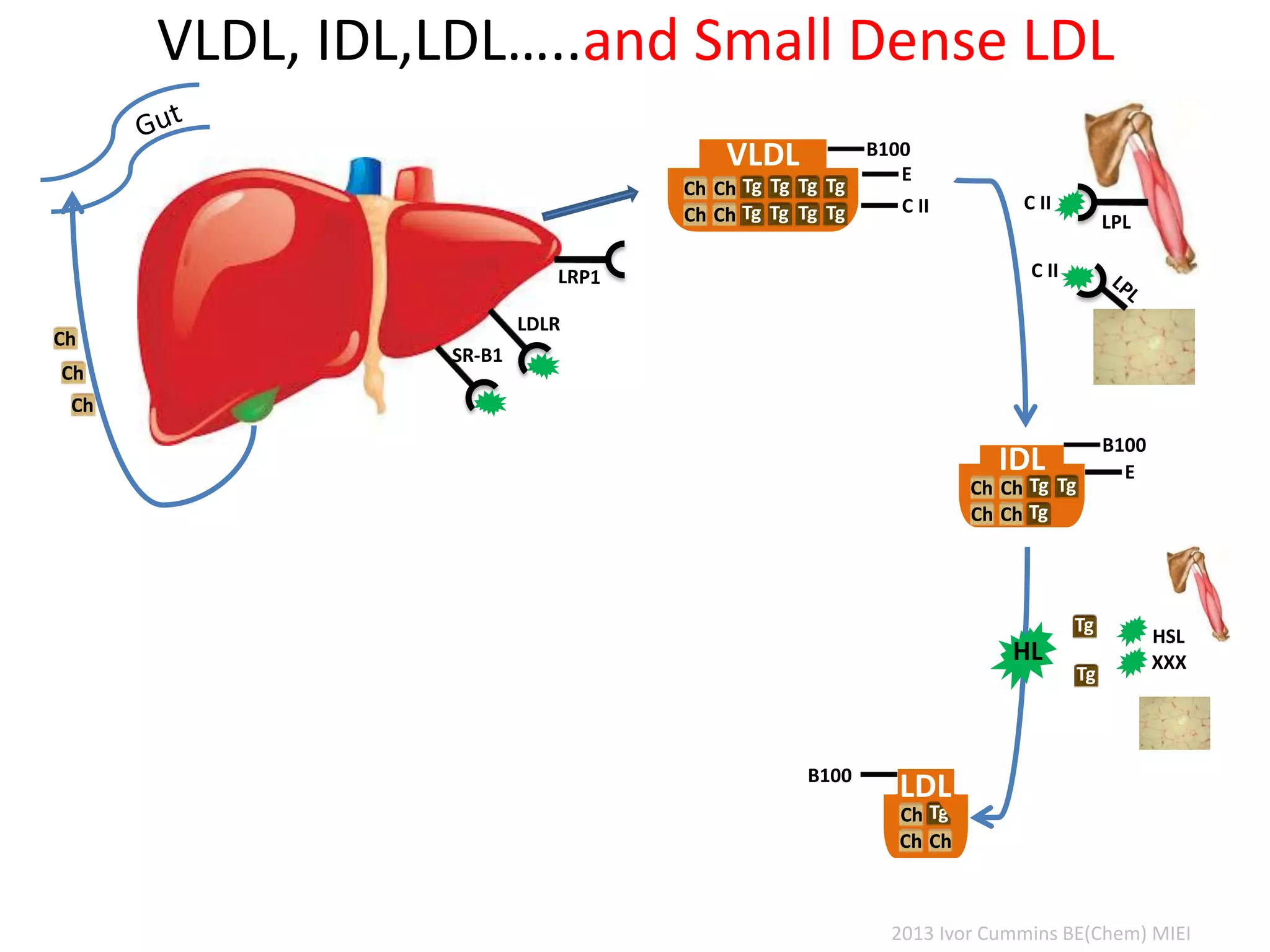
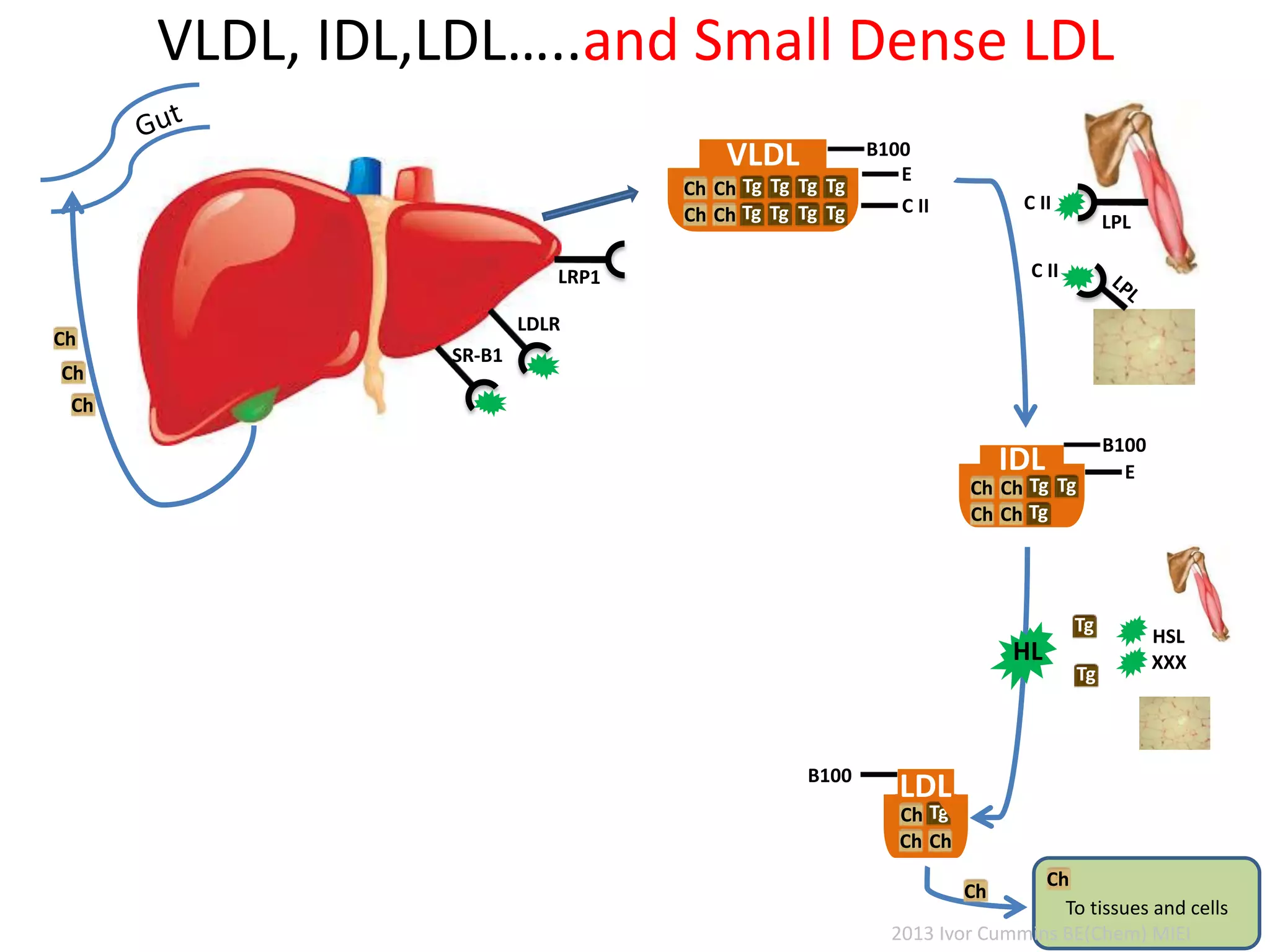
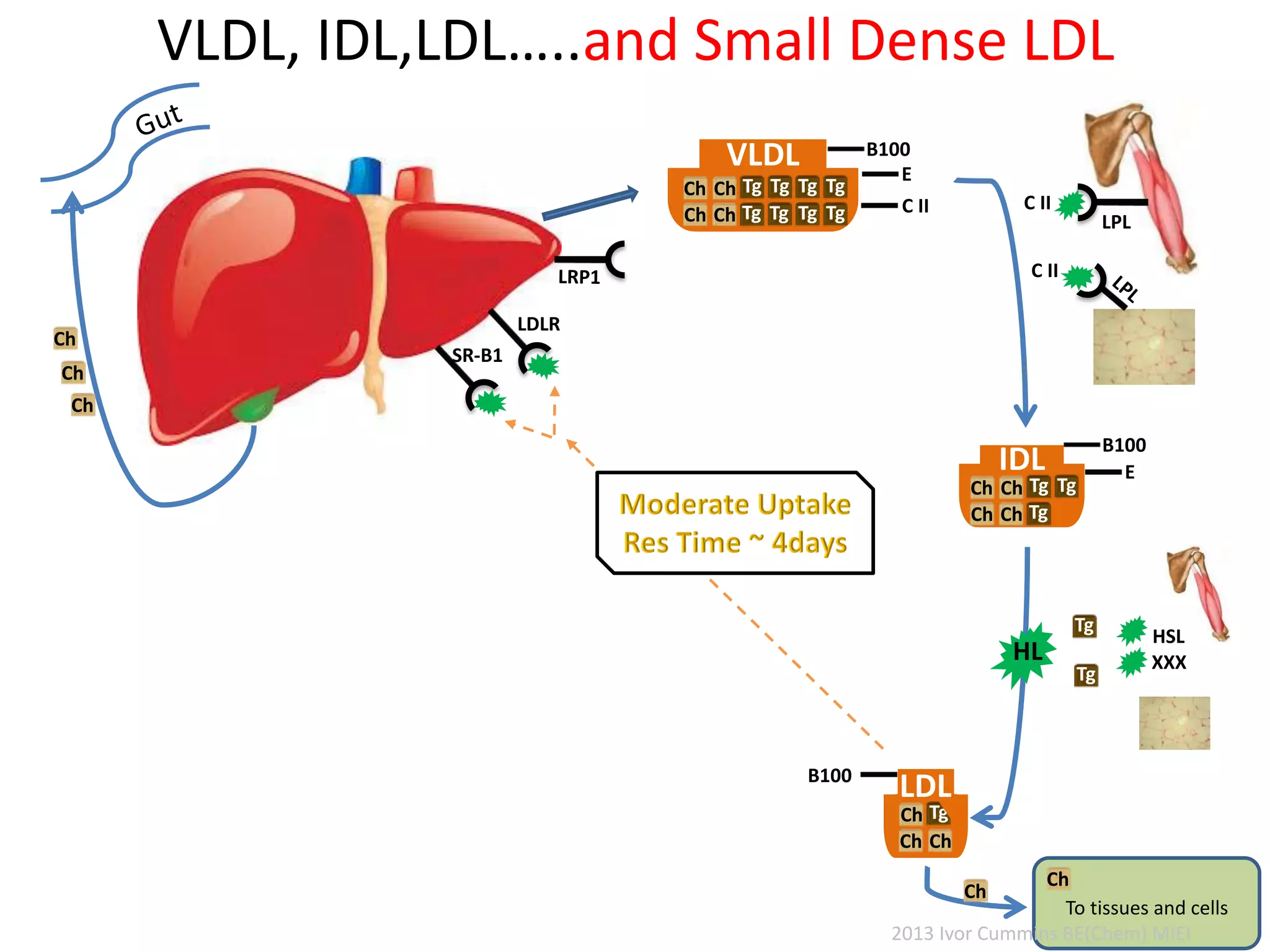
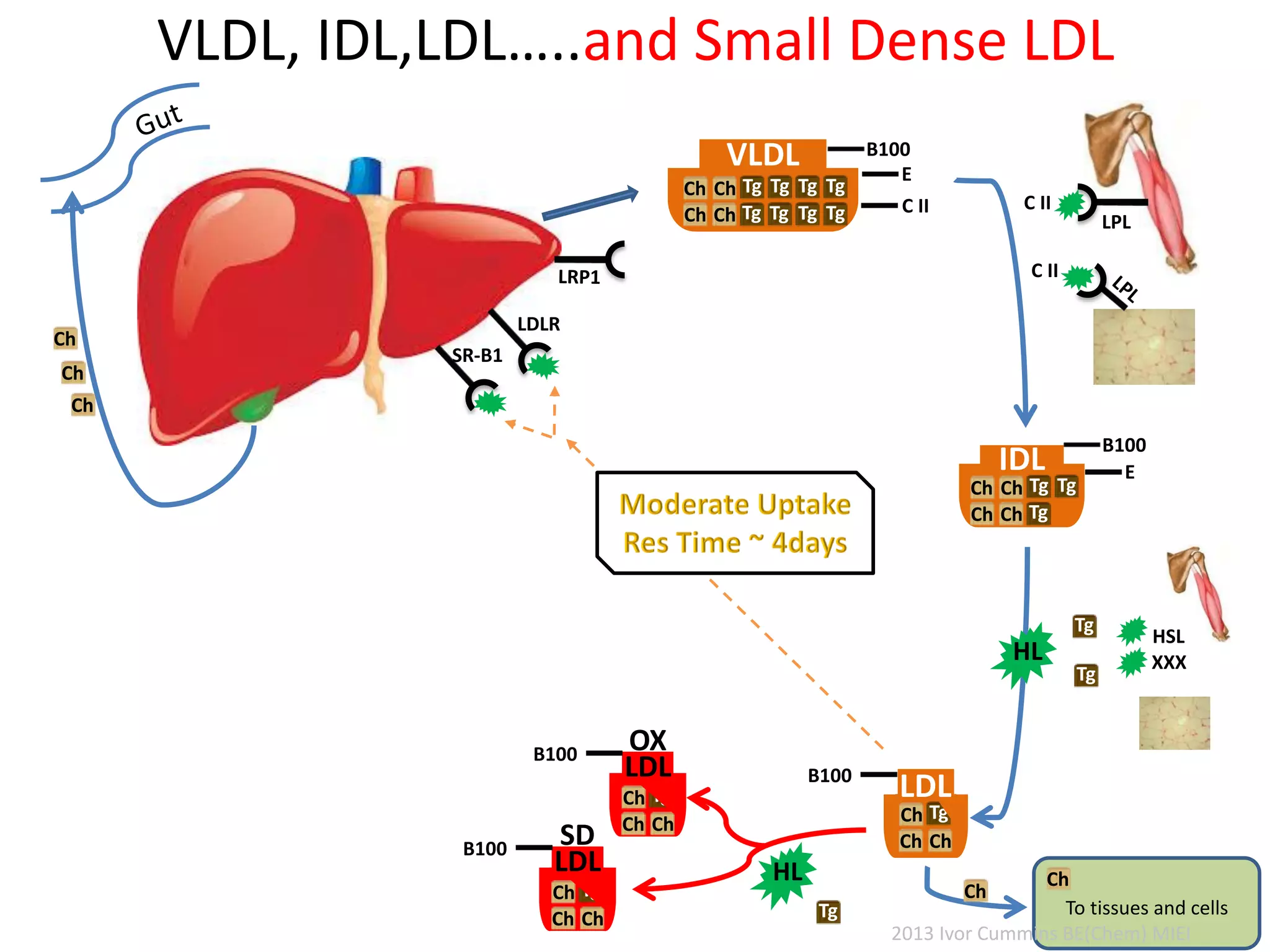
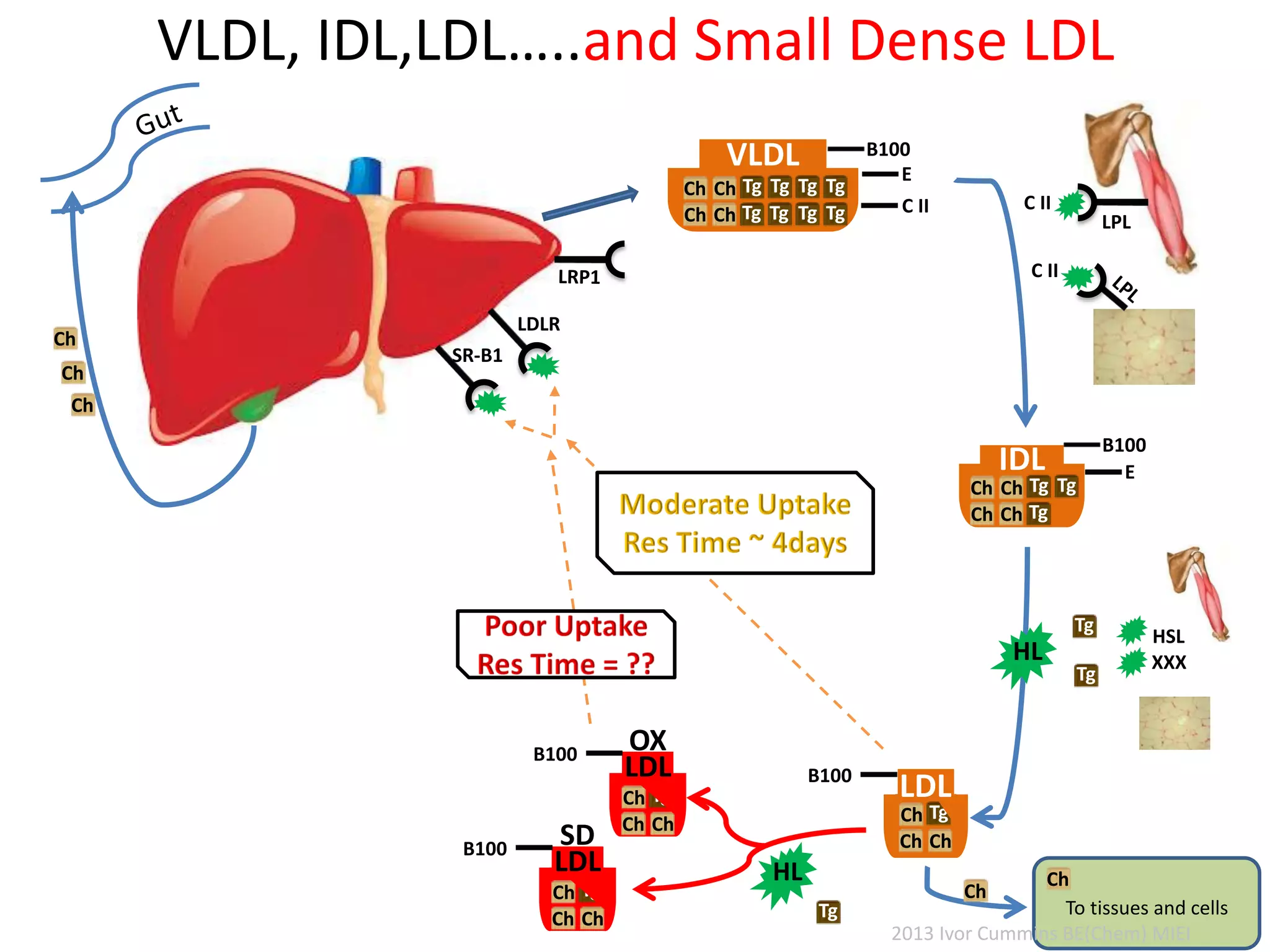
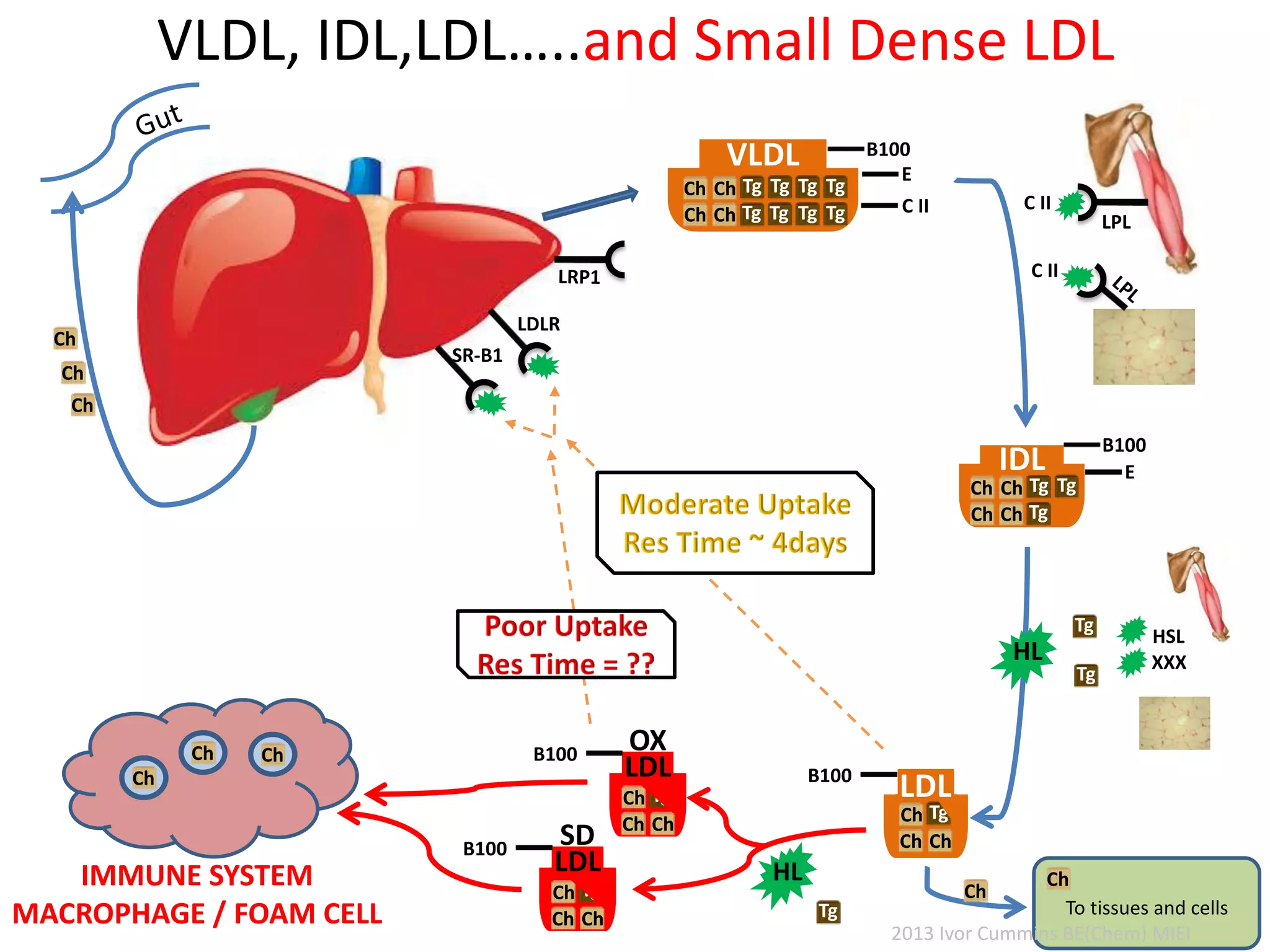
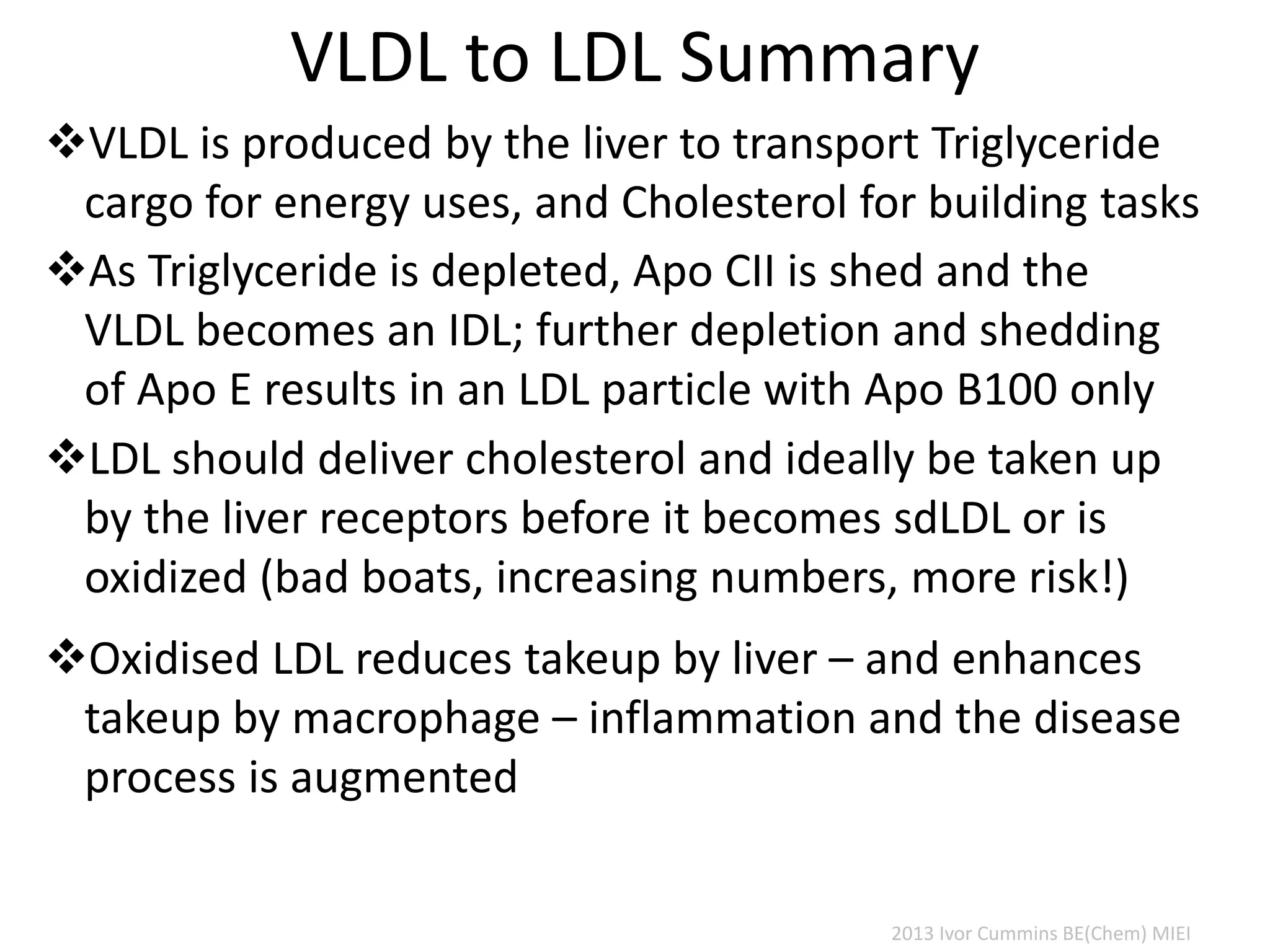
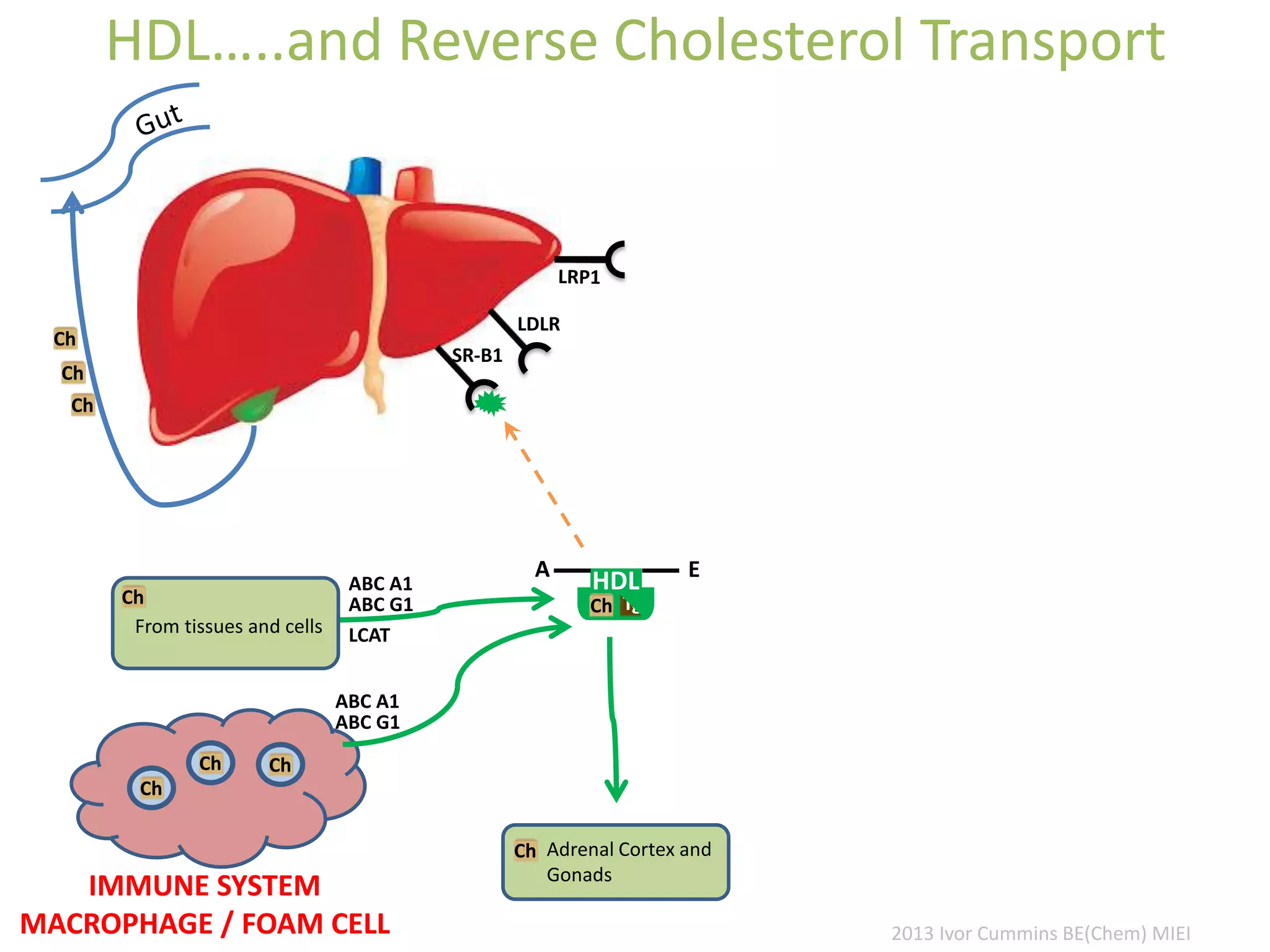
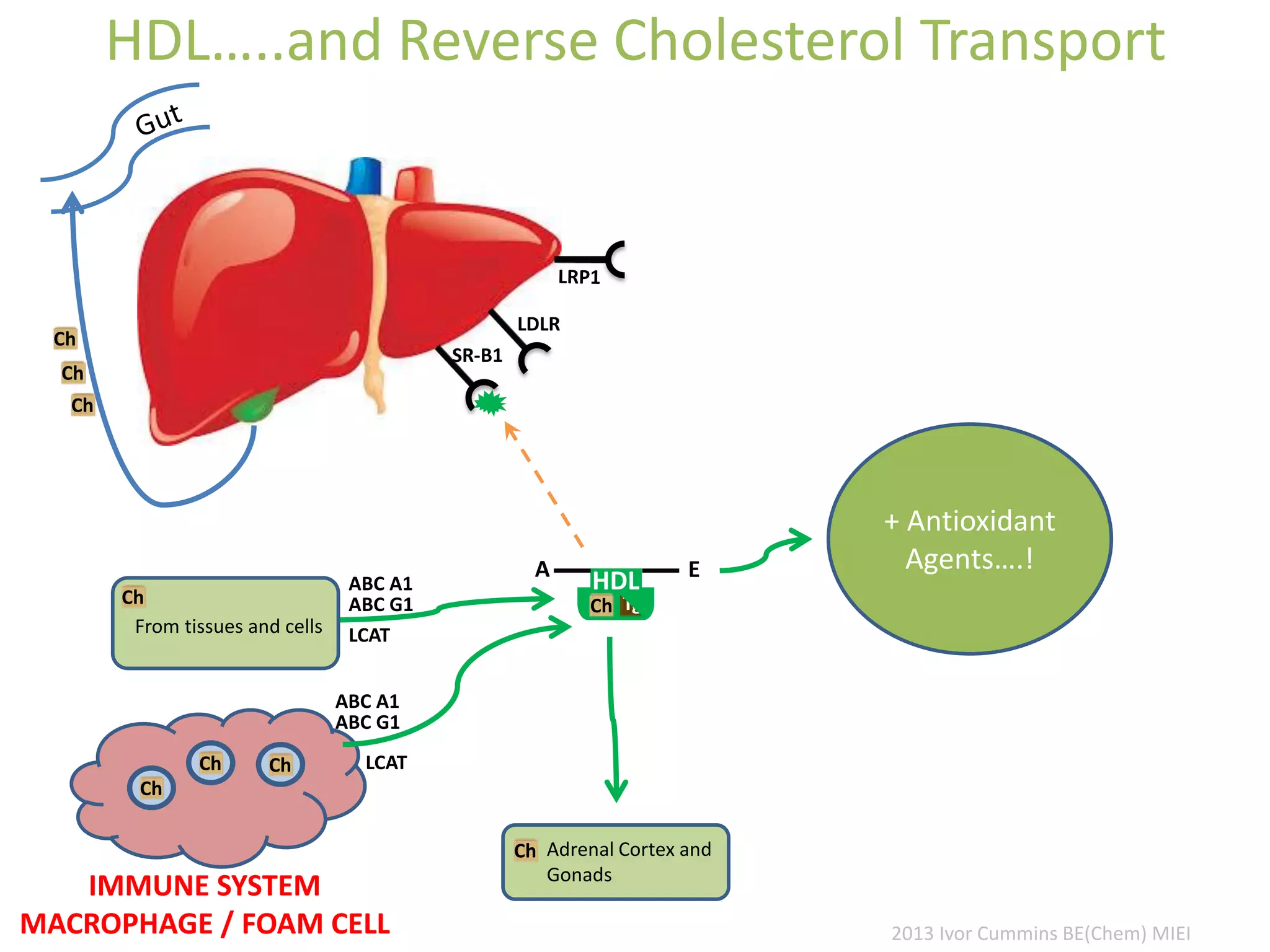
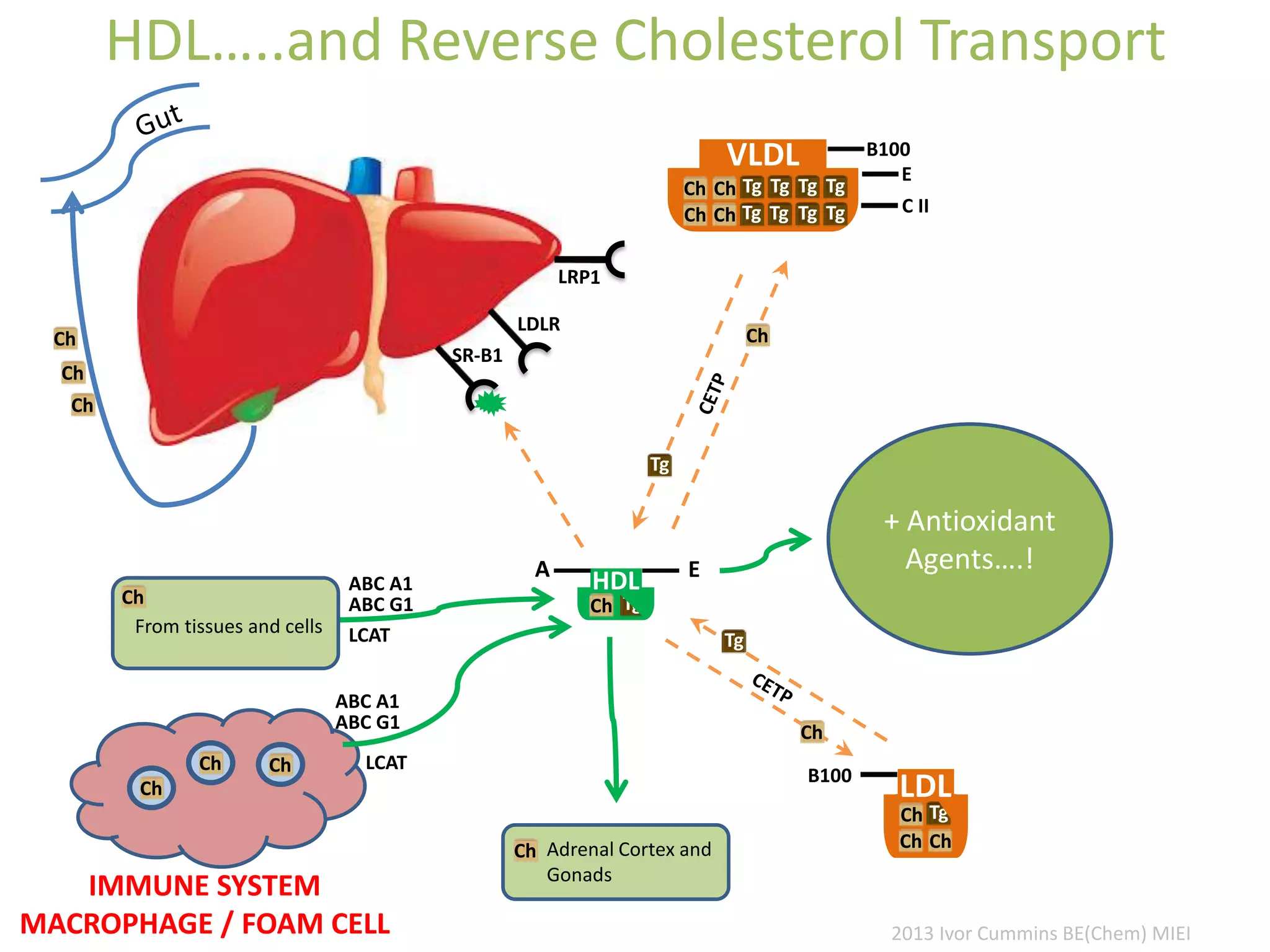
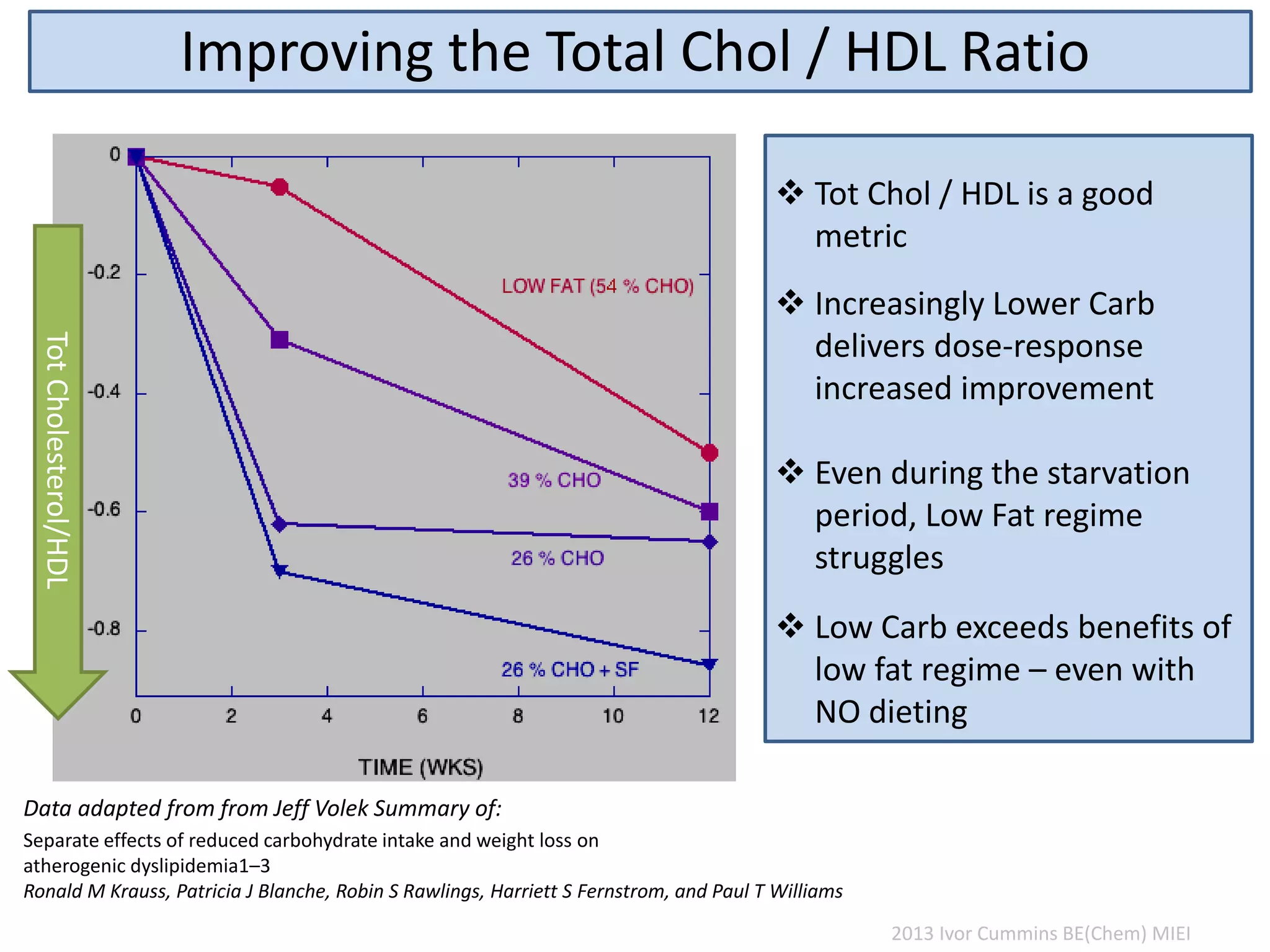
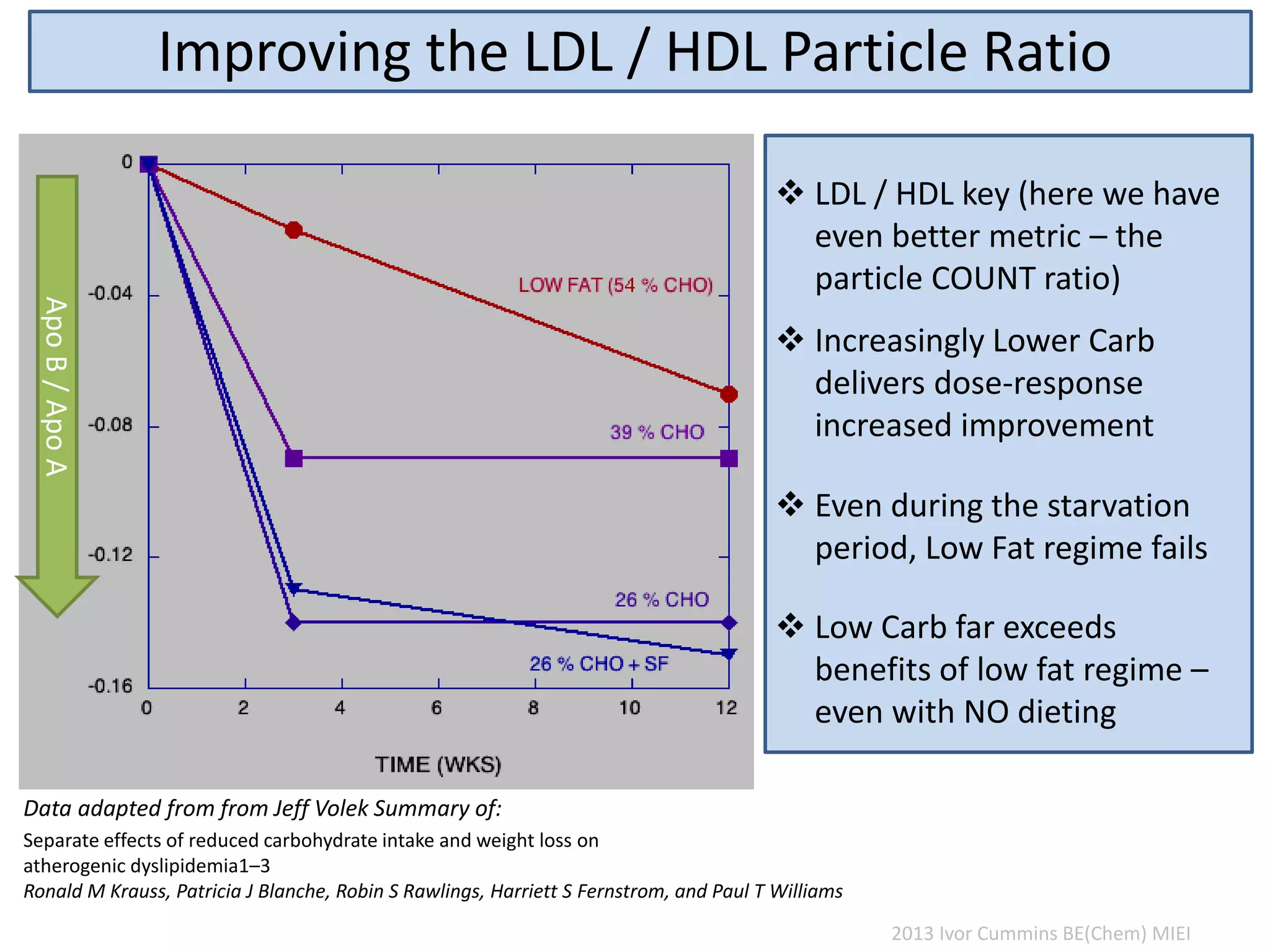
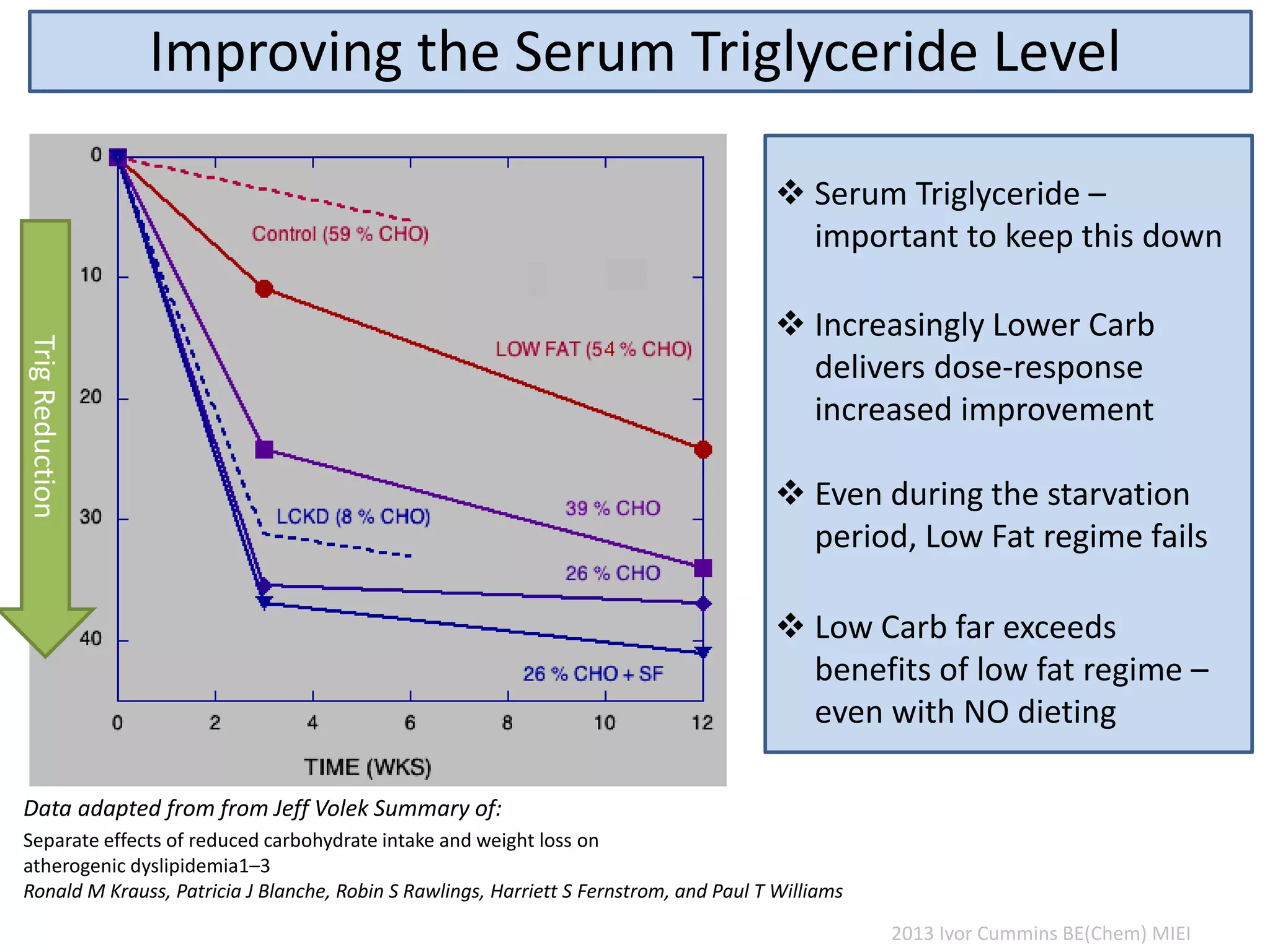
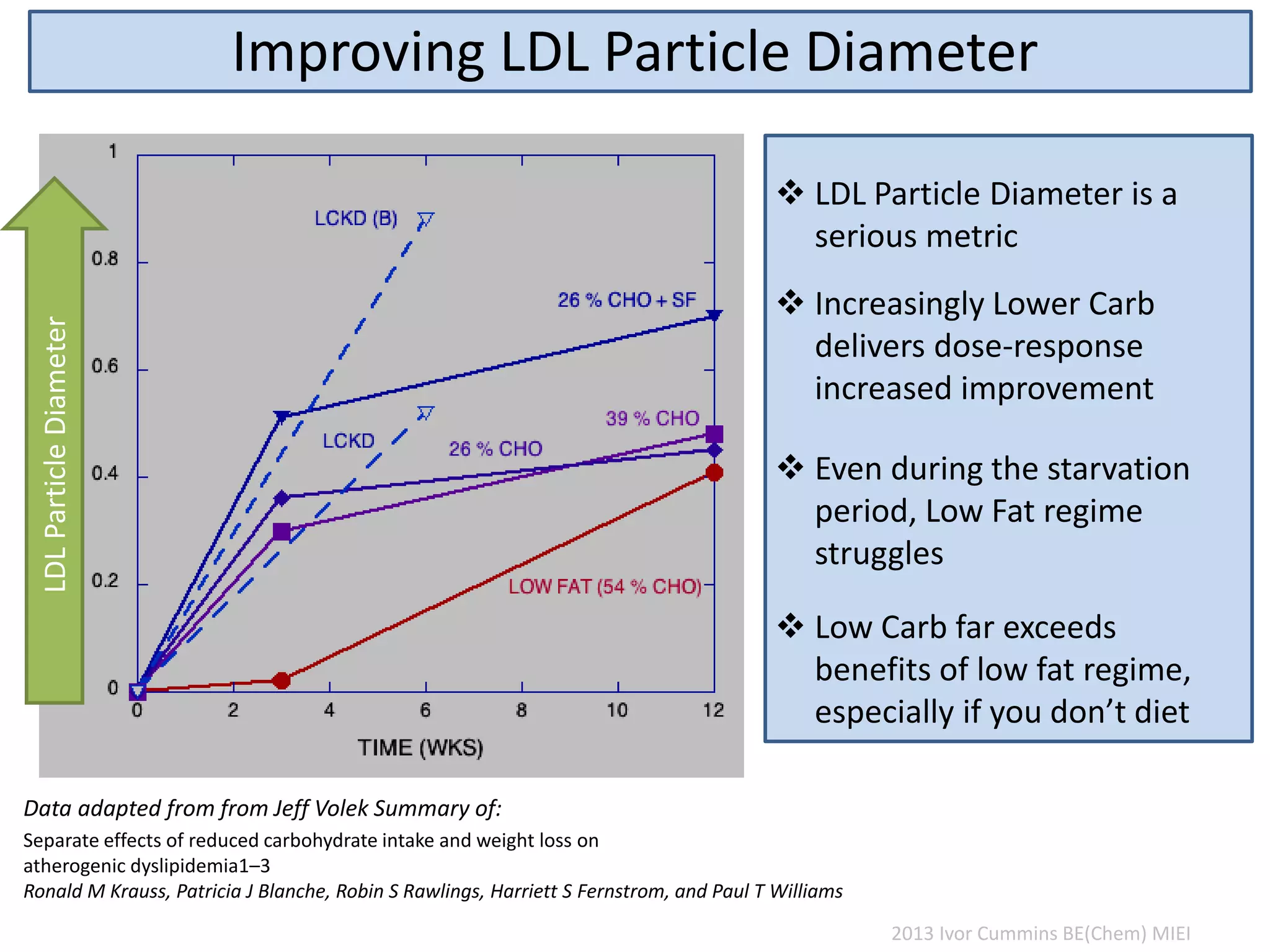
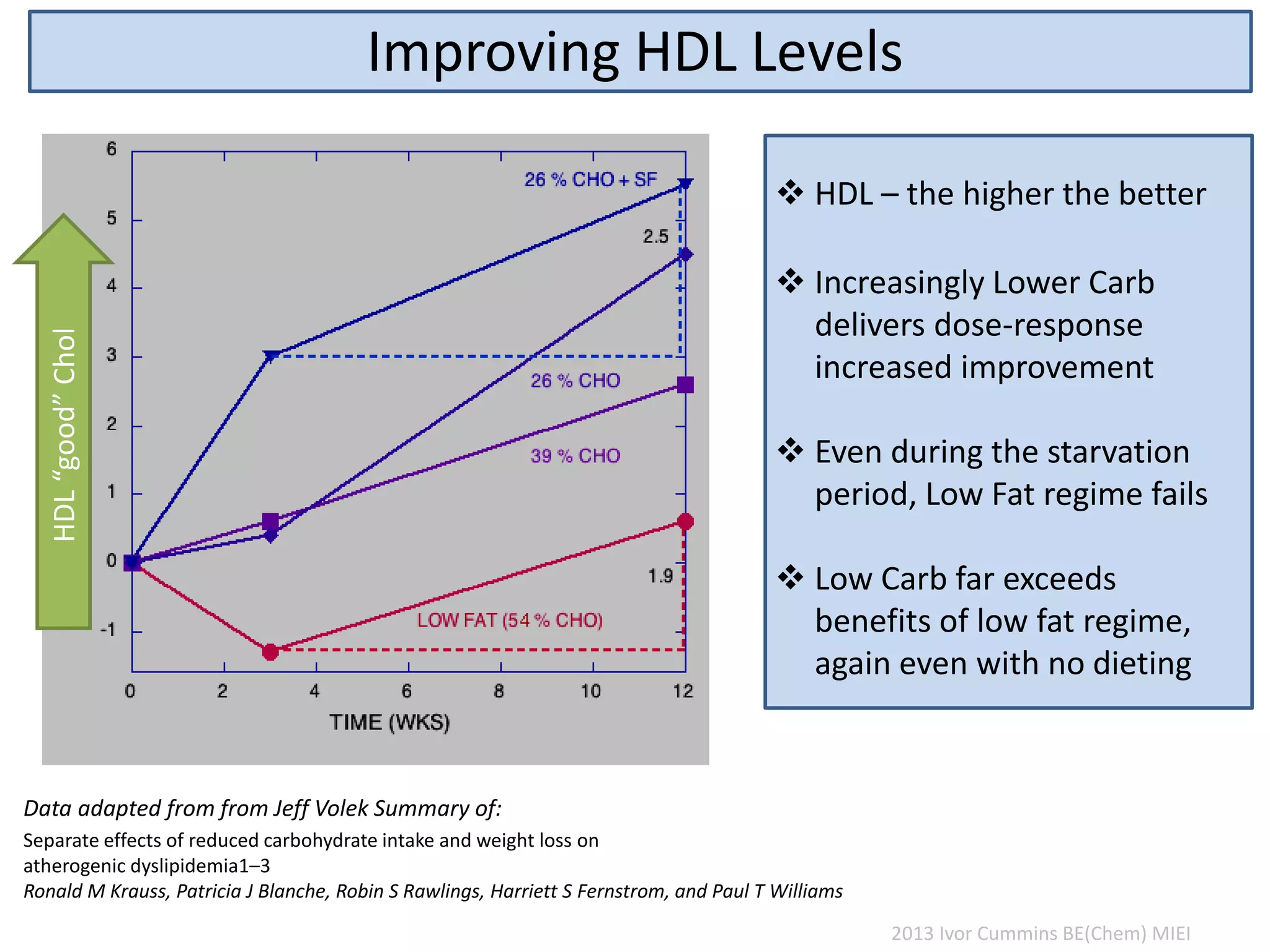
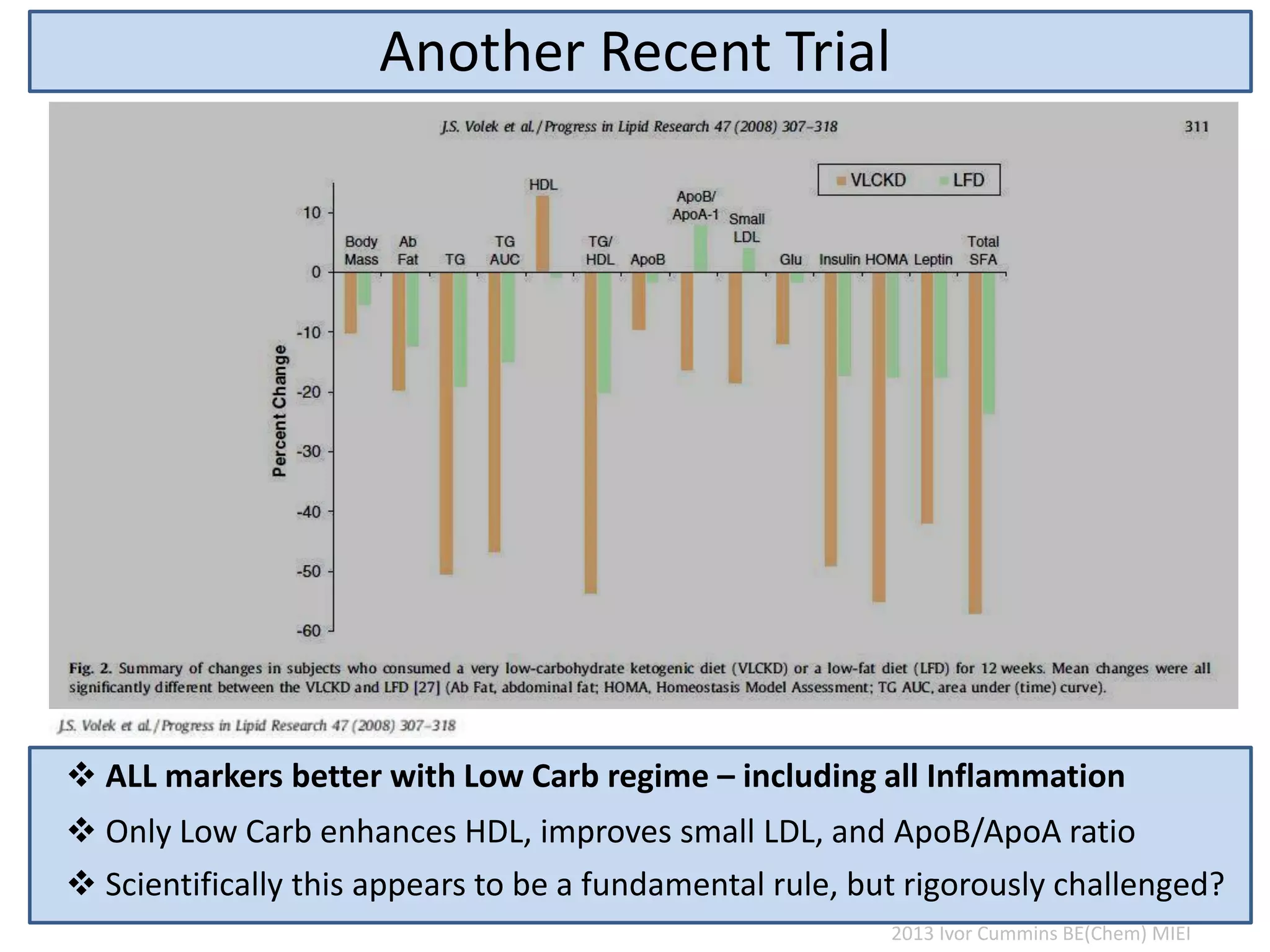
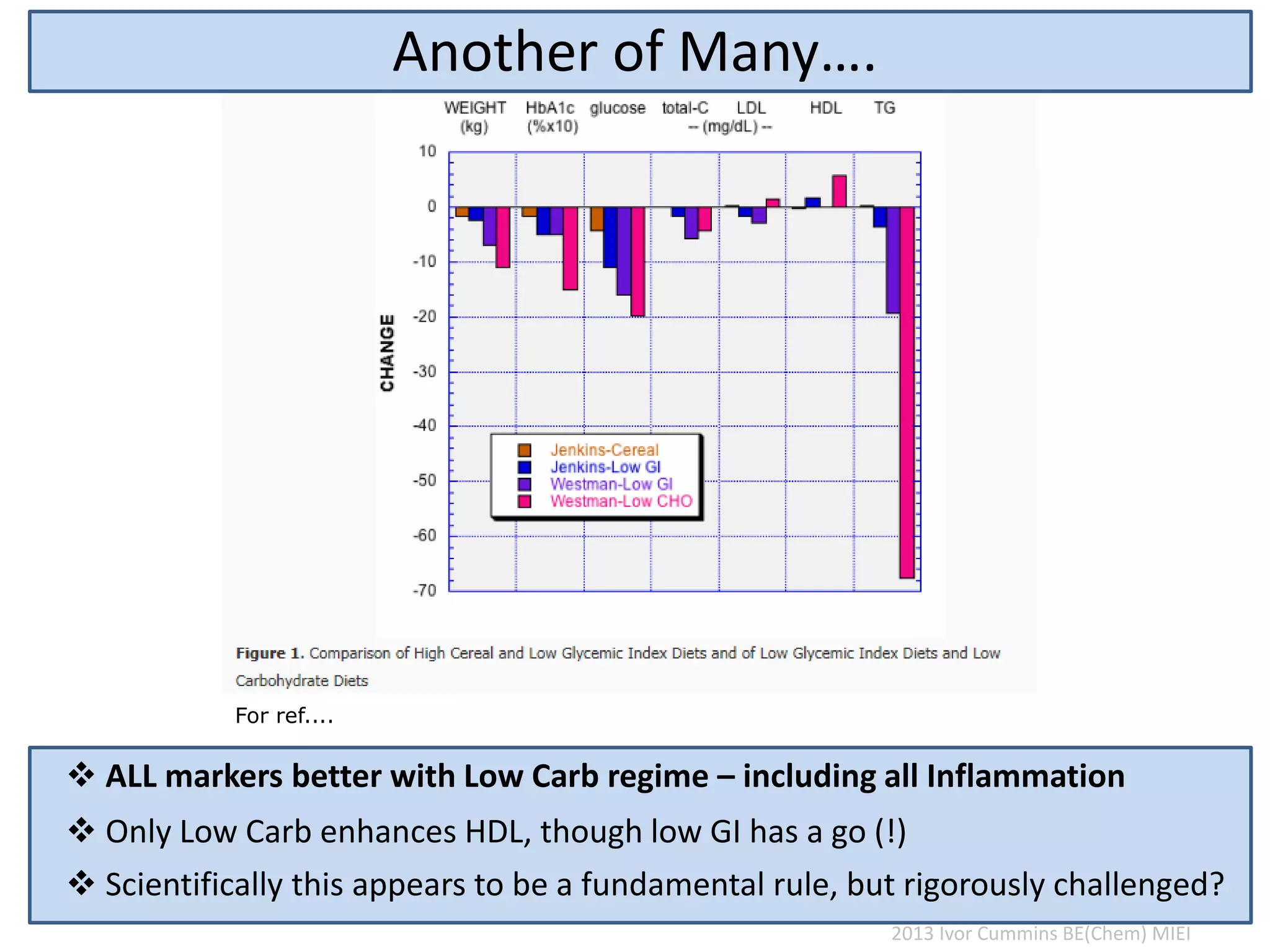
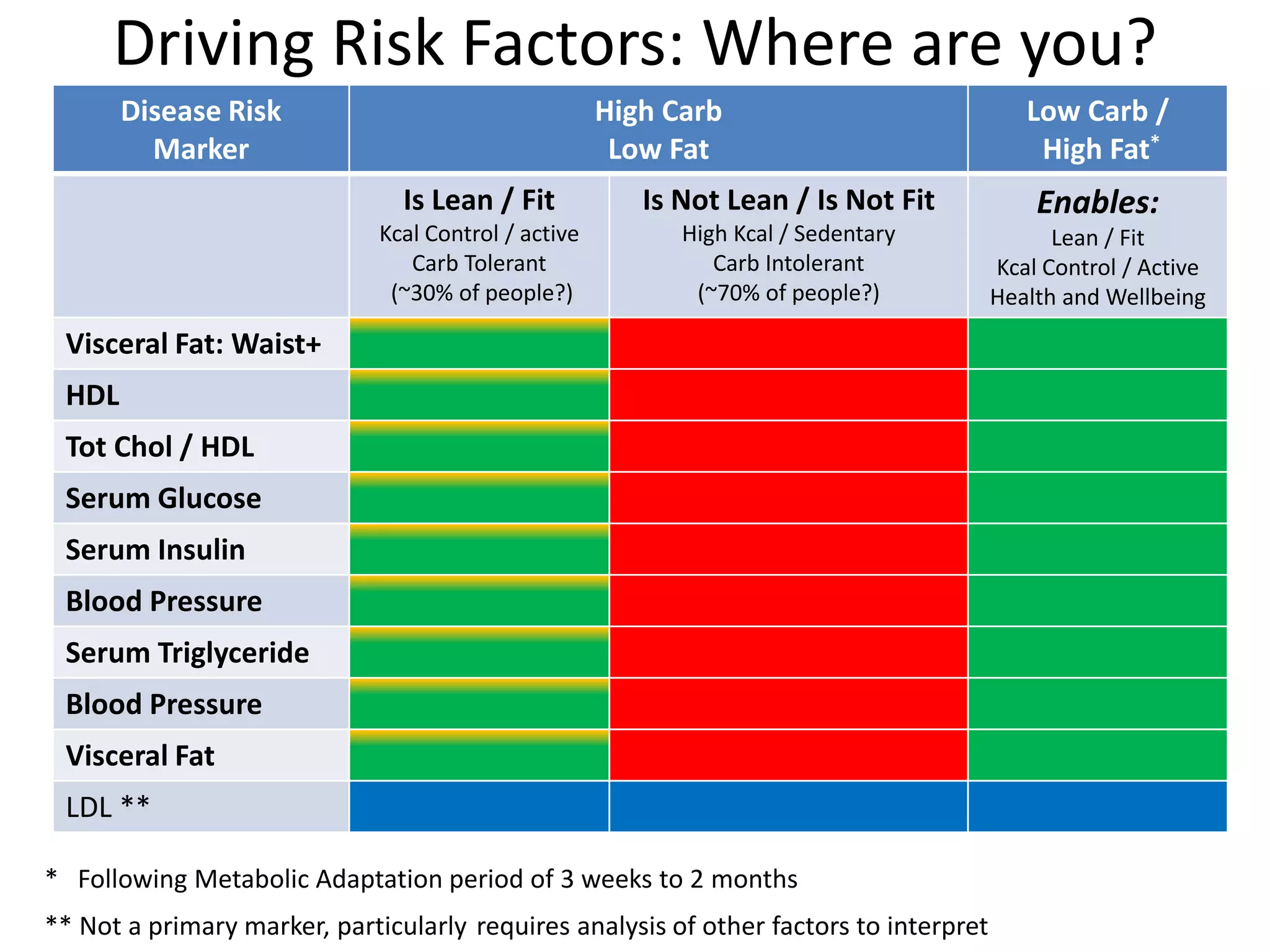

The document discusses the complexities of cholesterol, triglycerides, and their roles in health, emphasizing the importance of lipoproteins in transporting these molecules. It challenges traditional views on cholesterol as a primary risk factor for cardiovascular disease, arguing that factors like insulin resistance and specific lipoprotein types are more critical. A significant finding is the diminishing relevance of total cholesterol in predicting mortality risk, as supported by extensive research data.

























![Chemical Bonding [1]](https://cdn.slidesharecdn.com/ss_thumbnails/chemicalbonding1-100201094819-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)




























































