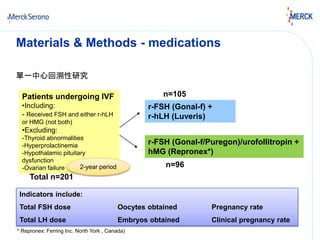
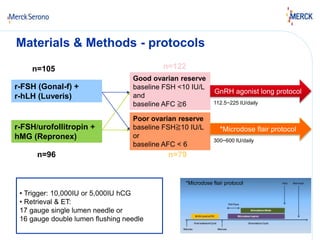
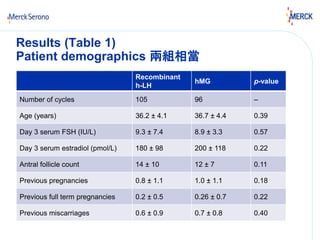
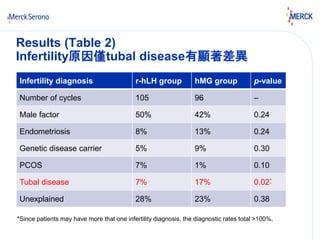
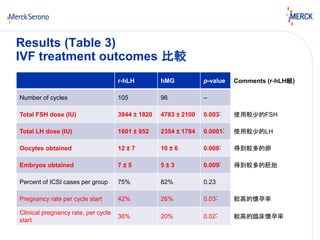
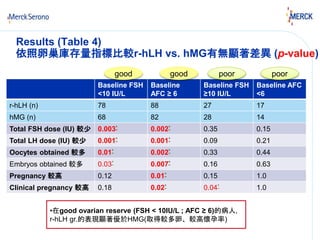
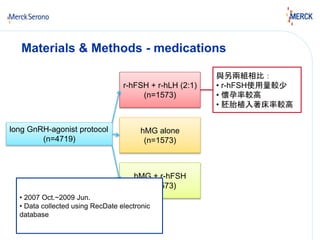
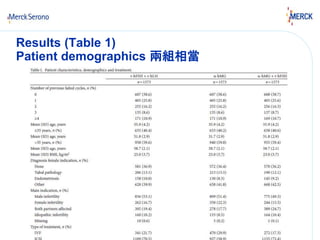
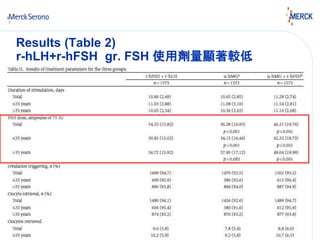
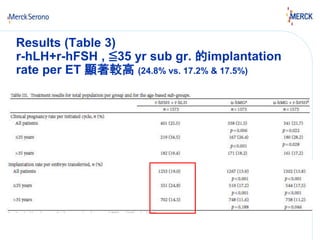
This study compared outcomes of IVF cycles stimulated with either recombinant LH (r-hLH) or human menopausal gonadotropins (hMG) acting as an LH analogue in subjects with good or poor ovarian reserve. The study found that in subjects with good ovarian reserve, as indicated by baseline FSH <10 IU/L and AFC ≥6, r-hLH resulted in significantly lower FSH dose, lower LH dose, higher oocyte yield, higher embryo yield, and higher pregnancy and clinical pregnancy rates compared to hMG. No significant differences were observed between r-hLH and hMG in subjects with poor ovarian reserve.