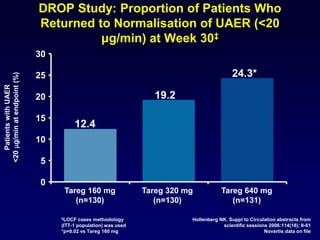
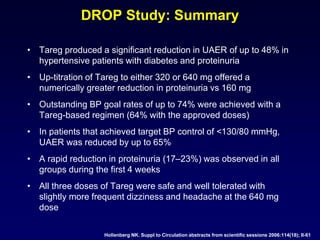
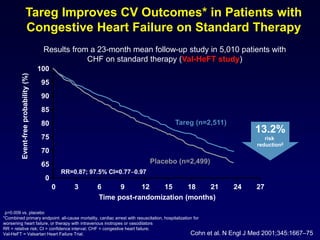
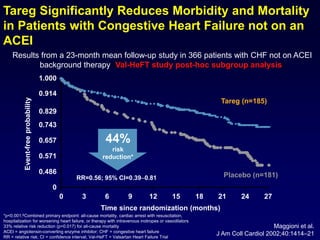
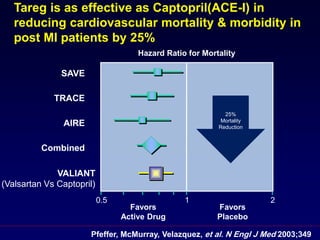
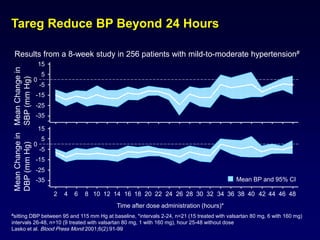
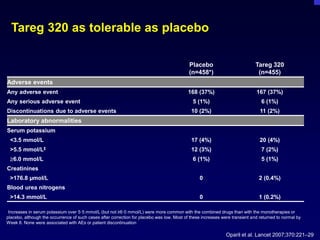
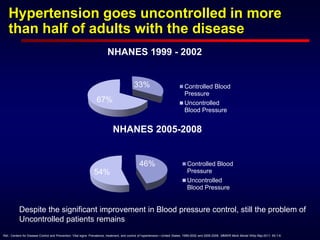
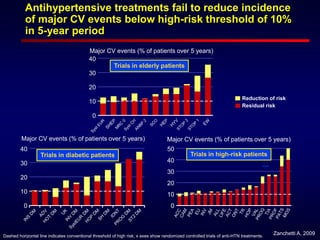
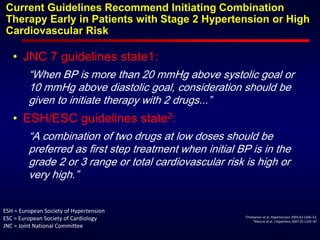
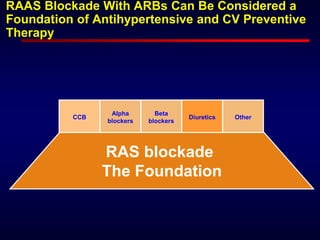
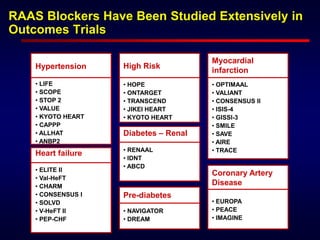
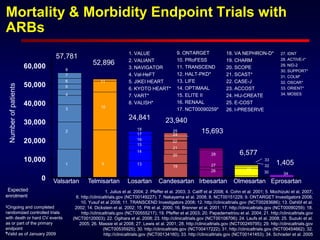
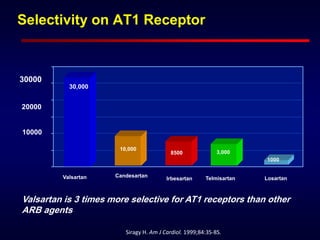
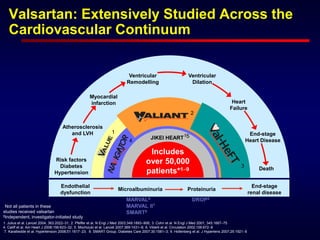
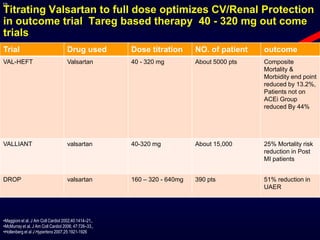
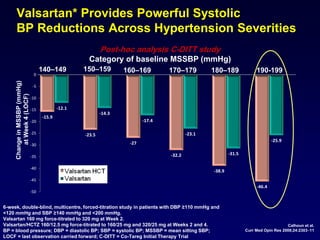
This document discusses hypertension and the need for high doses of antihypertensive medications. It provides data showing that over half of adults with hypertension still have uncontrolled blood pressure despite improvements. It also summarizes trials showing residual cardiovascular risk even when blood pressure is controlled. The document advocates for early use of combination antihypertensive therapy, especially those targeting the renin-angiotensin-aldosterone system, to improve control and reduce organ damage. It highlights valsartan specifically as a well-studied angiotensin receptor blocker with strong evidence from numerous trials across cardiovascular conditions.


![Proteinuria Is an Independent Risk Factor
for Mortality in Type 2 Diabetes
1.0
0.9
0.8
0.7
0.6
0.5
0 1 2 3 4 5 6
Years
Survival
(all-causemortality)
Normoalbuminuria
(n=191) [8%]
Microalbuminuria
(n=86) [20%]
Macroalbuminuria
(n=51) [35%]
Gall, MA et al. Diabetes 1995;44:1303
P<0.01 normo vs. micro- and macroalbuminuria
P<0.05 micro vs. macroalbuminuria](https://image.slidesharecdn.com/20-ueda2012dowestillneedhighdosesd-150629203957-lva1-app6891/85/ueda2012-do-we-still-need-high-doses-d-mohammed-27-320.jpg)