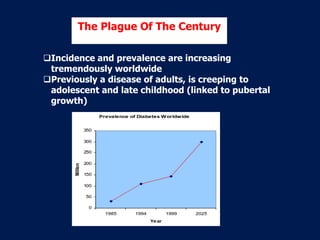
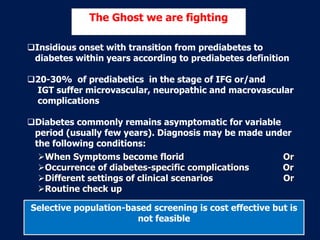
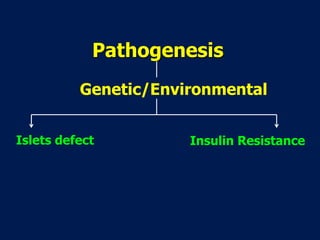
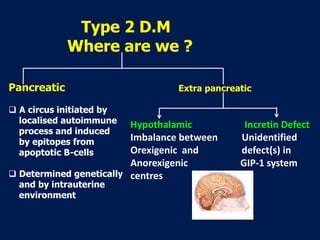
This document discusses type 2 diabetes, including its definition, pathogenesis, and current state of understanding. It defines type 2 diabetes as a group of metabolic disorders characterized by hyperglycemia due to defects in both insulin secretion and action. The document notes that type 2 diabetes is increasing worldwide and can now affect adolescents. It discusses the genetic and environmental factors involved in its pathogenesis, including islet cell defects and insulin resistance in tissues. While lifestyle changes and current pharmacotherapies can help manage the disease, the document concludes that the underlying mechanisms remain poorly understood and that type 2 diabetes continues to represent a major global health challenge.























































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)

