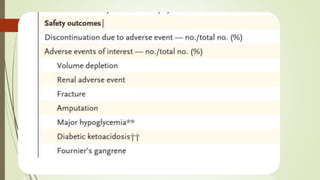
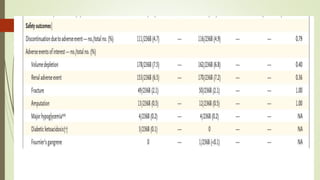
The DAPA-HF trial found that among patients with heart failure and reduced ejection fraction, those who received the SGLT2 inhibitor dapagliflozin had a lower risk of hospitalization for heart failure or cardiovascular death and better symptom scores compared to placebo, regardless of the presence of diabetes. Dapagliflozin reduced the primary composite outcome of worsening heart failure or cardiovascular death across subgroups. It provided cardiovascular benefits in patients without diabetes. Adverse effects were generally uncommon and less frequent with dapagliflozin.
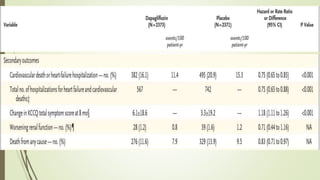
![ Secondary Outcomes
Total number of hospitalizations for heart failure (including repeat admissions) and
cardiovascular deaths;
Change from baseline to 8 months in the total symptom score on the Kansas City
Cardiomyopathy Questionnaire, which is scored on a scale from 0 to 100, with a higher
score indicating fewer symptoms and a change of 5 or more points considered to be
clinically meaningful.
A composite of worsening renal function, which was defined as a sustained decline in the
eGFR of 50% or greater, end-stage renal disease (defined as a sustained [≥28 days] eGFR
of <15 ml per minute per 1.73 m2 sustained dialysis, or renal transplantation), or renal
death;
And death from any cause.](https://image.slidesharecdn.com/journaldapagliflozin-copy-201015153313/85/Journal-dapagliflozin-dapahf-trial-15-320.jpg)